
Neonatal Nephrology/AKI 2
Session: Neonatal Nephrology/AKI 2
 photo")
Timothy Nelin, MD (he/him/his)
Attending Physician
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
.png)
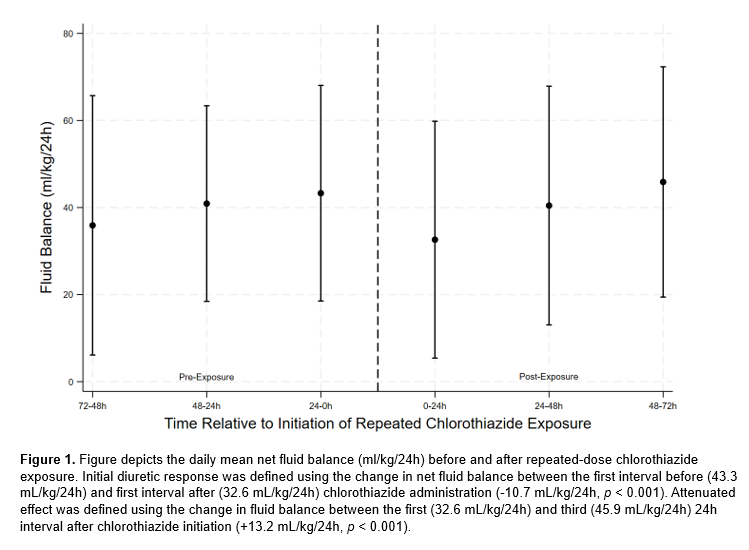 Figure depicts the daily mean net fluid balance (ml/kg/24h) before and after repeated-dose chlorothiazide exposure. Initial diuretic response was defined using the change in net fluid balance between the first interval before (43.3 mL/kg/24h) and first interval after (32.6 mL/kg/24h) chlorothiazide administration (-10.7 mL/kg/24h, p < 0.001). Attenuated effect was defined using the change in fluid balance between the first (32.6 mL/kg/24h) and third (45.9 mL/kg/24h) 24h interval after chlorothiazide initiation (+13.2 mL/kg/24h, p < 0.001).
Figure depicts the daily mean net fluid balance (ml/kg/24h) before and after repeated-dose chlorothiazide exposure. Initial diuretic response was defined using the change in net fluid balance between the first interval before (43.3 mL/kg/24h) and first interval after (32.6 mL/kg/24h) chlorothiazide administration (-10.7 mL/kg/24h, p < 0.001). Attenuated effect was defined using the change in fluid balance between the first (32.6 mL/kg/24h) and third (45.9 mL/kg/24h) 24h interval after chlorothiazide initiation (+13.2 mL/kg/24h, p < 0.001).  Figure depicts the daily mean net fluid balance (ml/kg/24h) before and after repeated-dose chlorothiazide exposure. Initial diuretic response was defined using the change in net fluid balance between the first interval before (43.3 mL/kg/24h) and first interval after (32.6 mL/kg/24h) chlorothiazide administration (-10.7 mL/kg/24h, p < 0.001). Attenuated effect was defined using the change in fluid balance between the first (32.6 mL/kg/24h) and third (45.9 mL/kg/24h) 24h interval after chlorothiazide initiation (+13.2 mL/kg/24h, p < 0.001).
Figure depicts the daily mean net fluid balance (ml/kg/24h) before and after repeated-dose chlorothiazide exposure. Initial diuretic response was defined using the change in net fluid balance between the first interval before (43.3 mL/kg/24h) and first interval after (32.6 mL/kg/24h) chlorothiazide administration (-10.7 mL/kg/24h, p < 0.001). Attenuated effect was defined using the change in fluid balance between the first (32.6 mL/kg/24h) and third (45.9 mL/kg/24h) 24h interval after chlorothiazide initiation (+13.2 mL/kg/24h, p < 0.001). 