
Emergency Medicine 6
Session: Emergency Medicine 6
 Credit")
 photo")
Abbigayle K. Carlson, DO (she/her/hers)
Resident
Children's Mercy Hospitals and Clinics
Overland Park, Kansas, United States
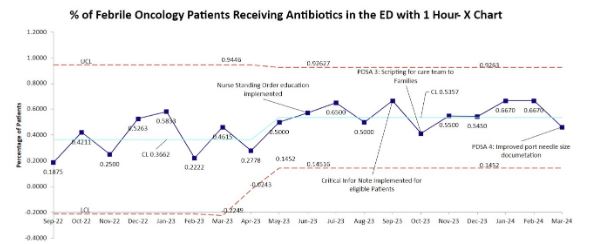 Percentage of ED febrile oncology patients with antibiotics < 60 min
Percentage of ED febrile oncology patients with antibiotics < 60 min 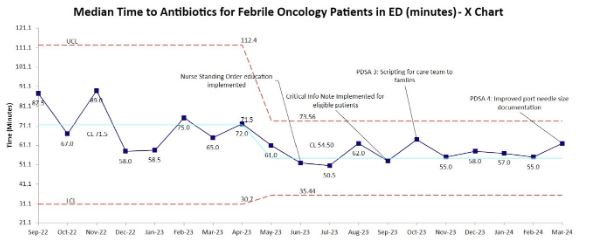 Median time to antibiotics in febrile oncology ED patients.
Median time to antibiotics in febrile oncology ED patients. 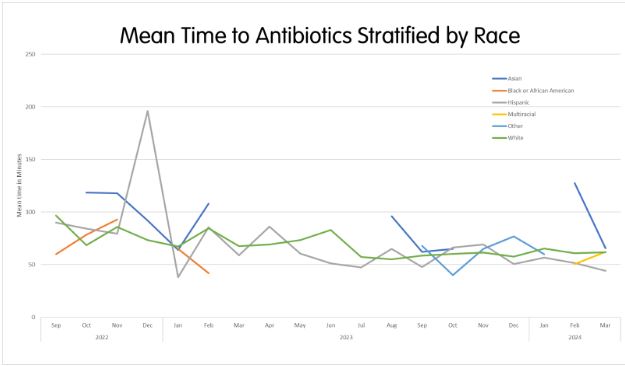 Time to antibiotics stratified by race/ethnicityPercentage of ED febrile oncology patients with antibiotics < 60 min Median time to antibiotics in febrile oncology ED patients. Time to antibiotics stratified by race/ethnicity
Time to antibiotics stratified by race/ethnicityPercentage of ED febrile oncology patients with antibiotics < 60 min Median time to antibiotics in febrile oncology ED patients. Time to antibiotics stratified by race/ethnicity