
Neonatal Quality Improvement 6
Session: Neonatal Quality Improvement 6
 Credit")
 photo")
Shelbye Schweinhart, MD (she/her/hers)
Neonatal Fellow
University of Louisville School of Medicine
Louisville, Kentucky, United States
.png) NICU postpartum depression screening increased from 0% to 59% over the initial project timeline. Key interventions are highlighted.
NICU postpartum depression screening increased from 0% to 59% over the initial project timeline. Key interventions are highlighted. 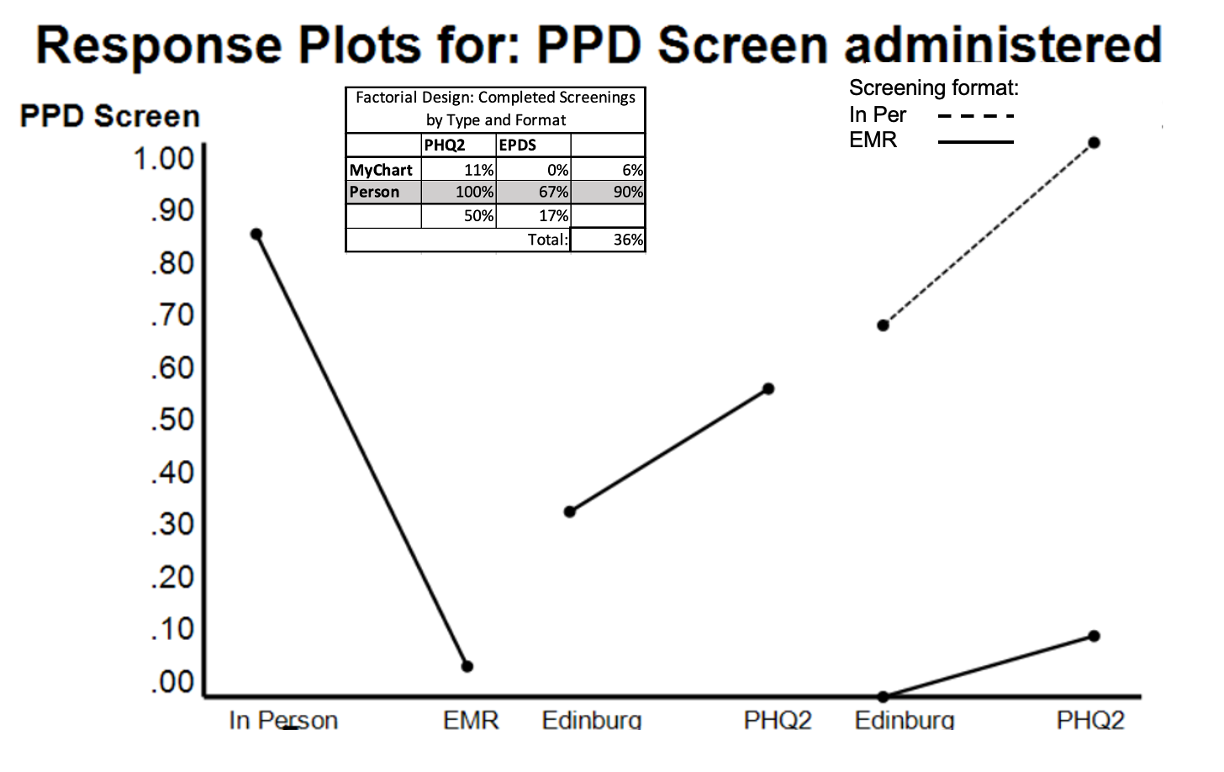 Our initial testing showed a significant negative effect of utilizing EMR communication to screen NICU caregivers without a significant effect of screener type. There was no significant interaction between factors tested.
Our initial testing showed a significant negative effect of utilizing EMR communication to screen NICU caregivers without a significant effect of screener type. There was no significant interaction between factors tested. .png) Chart showing comparison of percentage of completed screens over time for total eligible to segmented groups. Overall, similar screening rates were achieved across groups.
Chart showing comparison of percentage of completed screens over time for total eligible to segmented groups. Overall, similar screening rates were achieved across groups. 