
Neonatal Quality Improvement 4
Session: Neonatal Quality Improvement 4
 Credit")
 photo")
Carmen A. Alvarez Gell, MD (she/her/hers)
Pediatric Resident
The Children's Hospital at Montefiore
Bronx, New York, United States
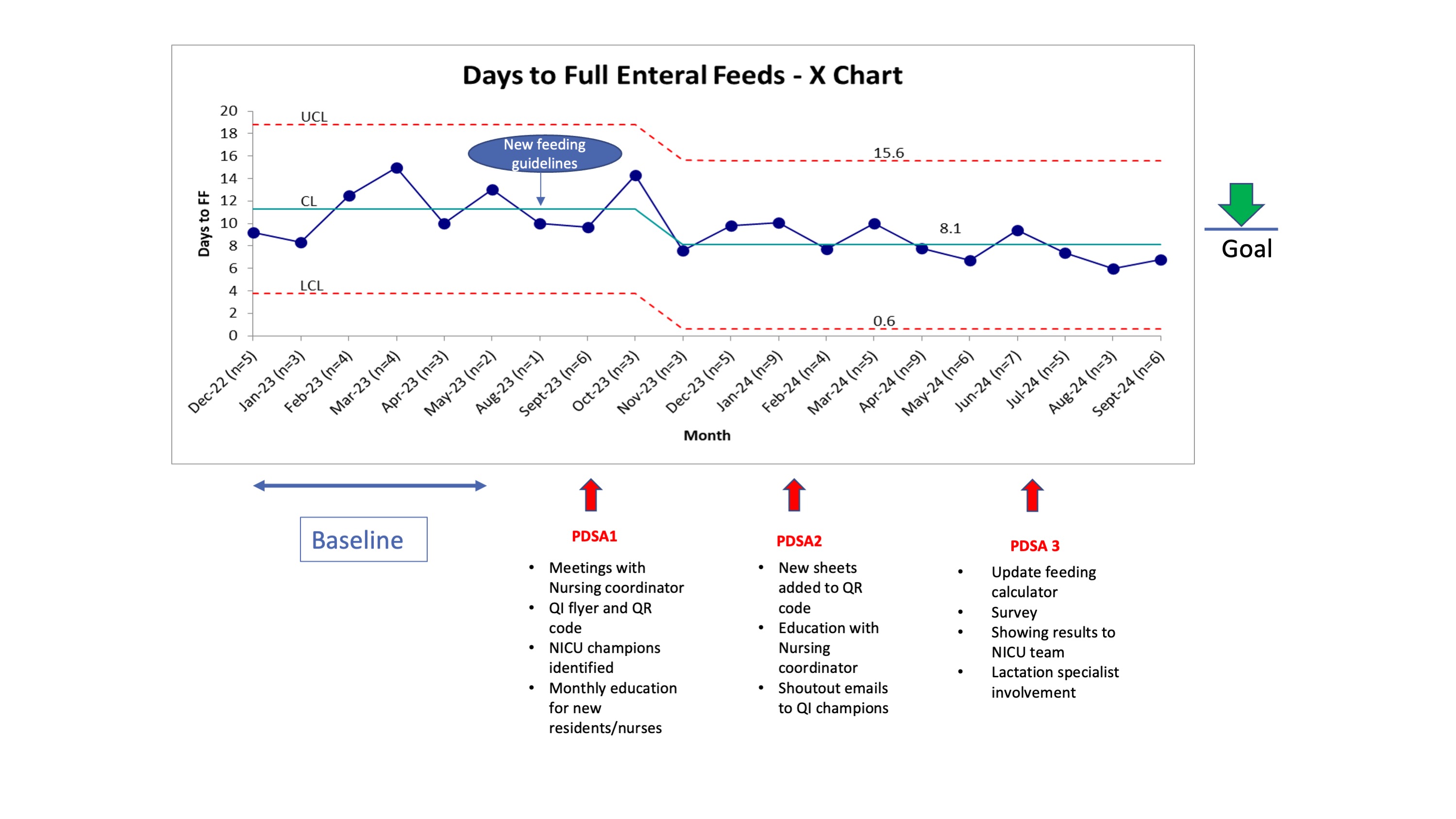 Statistical control chart of days to full enteral feeds by month with shift from baseline of a mean (blue center line) of 11.3 days per eligible infant to 8.1 days (28% decrease from baseline). UCL=upper control limit, LCL=lower control limit.
Statistical control chart of days to full enteral feeds by month with shift from baseline of a mean (blue center line) of 11.3 days per eligible infant to 8.1 days (28% decrease from baseline). UCL=upper control limit, LCL=lower control limit.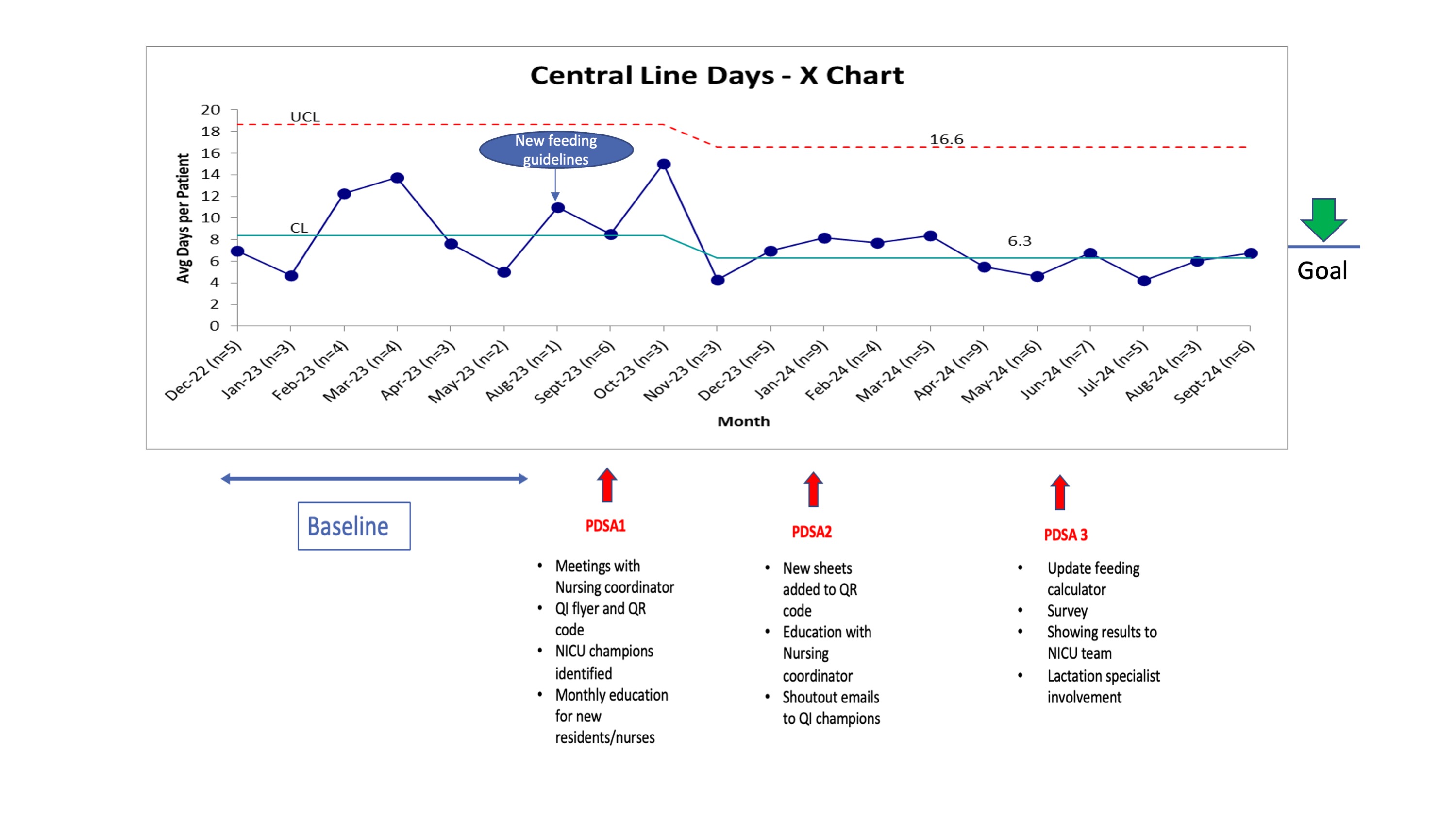 Statistical control chart of central line days by month with shift from baseline of a mean (blue center line) of 8.4 days per eligible infant to 6.3 days (25% decrease from baseline).
Statistical control chart of central line days by month with shift from baseline of a mean (blue center line) of 8.4 days per eligible infant to 6.3 days (25% decrease from baseline). 