
Neonatal Nephrology/AKI 1
Session: Neonatal Nephrology/AKI 1
 photo")
Elliott Huang, MD MPH (he/him/his)
Clinical Postdoctoral Fellow
Columbia University Vagelos College of Physicians and Surgeons
New York, New York, United States
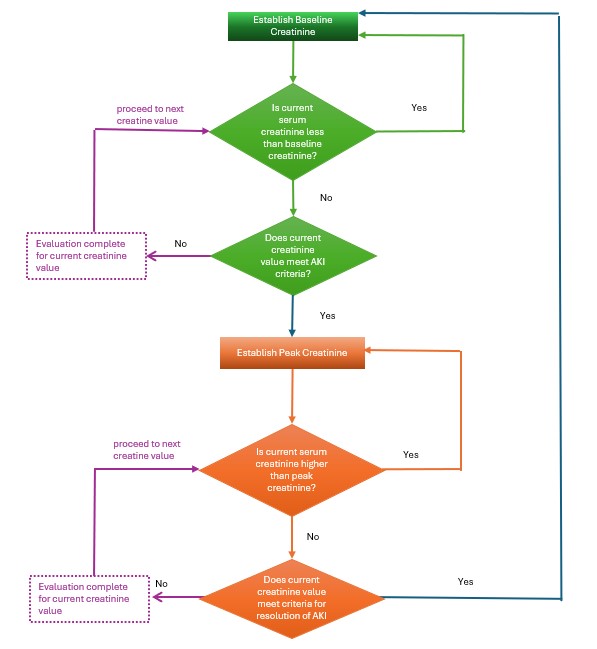 Visual demonstration of the steps for identifying AKI and resolution for each serum creatinine value.
Visual demonstration of the steps for identifying AKI and resolution for each serum creatinine value..png) Number of AKI events by gestational age and sex.
Number of AKI events by gestational age and sex.