
Hematology/Oncology 2: Pediatric Hematology
Session: Hematology/Oncology 2: Pediatric Hematology
 photo")
Kemar V. Prussien, PhD (she/her/hers)
Assistant Professor
Children's Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
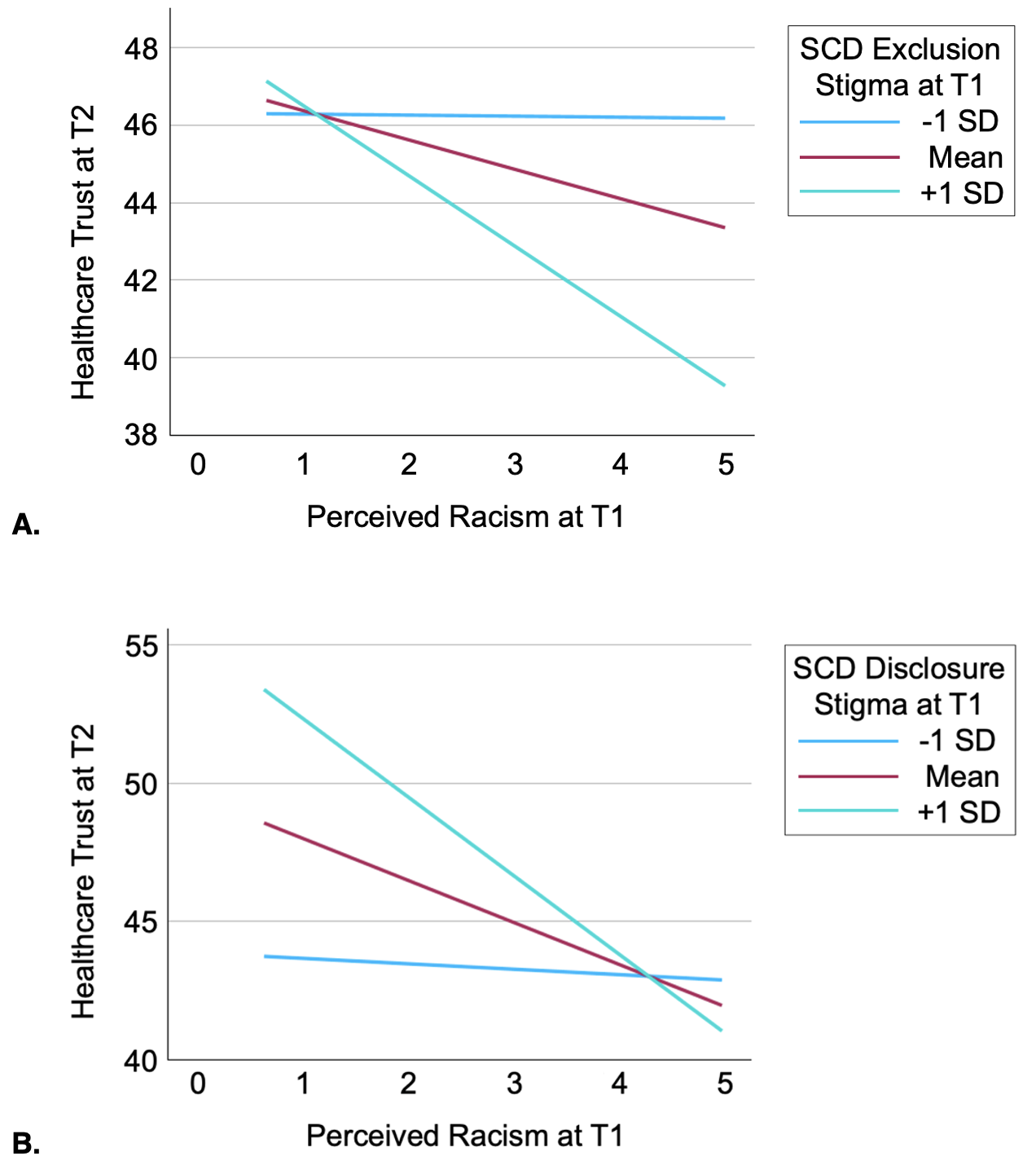 A. Line graph of the interaction between perceived racism and SCD exclusion stigma predicting healthcare trust. Simple slopes are depicted for AYA 1 SD below the mean reported exclusion stigma level (B = -.03, p = .974), at the mean reported exclusion stigma level (B = -.74, p = .236), and 1 SD above the mean exclusion stigma level (B = -1.80, p = .009). B. Line graph of the interaction between perceived racism and SCD disclosure stigma predicting healthcare trust. Simple slopes are depicted for AYA 1 SD below the mean reported disclosure stigma level (B = -.20, p = .834), at the mean reported disclosure stigma level (B = -1.51, p = .018), and 1 SD above the mean disclosure stigma level (B = -2.83, p < .001).
A. Line graph of the interaction between perceived racism and SCD exclusion stigma predicting healthcare trust. Simple slopes are depicted for AYA 1 SD below the mean reported exclusion stigma level (B = -.03, p = .974), at the mean reported exclusion stigma level (B = -.74, p = .236), and 1 SD above the mean exclusion stigma level (B = -1.80, p = .009). B. Line graph of the interaction between perceived racism and SCD disclosure stigma predicting healthcare trust. Simple slopes are depicted for AYA 1 SD below the mean reported disclosure stigma level (B = -.20, p = .834), at the mean reported disclosure stigma level (B = -1.51, p = .018), and 1 SD above the mean disclosure stigma level (B = -2.83, p < .001).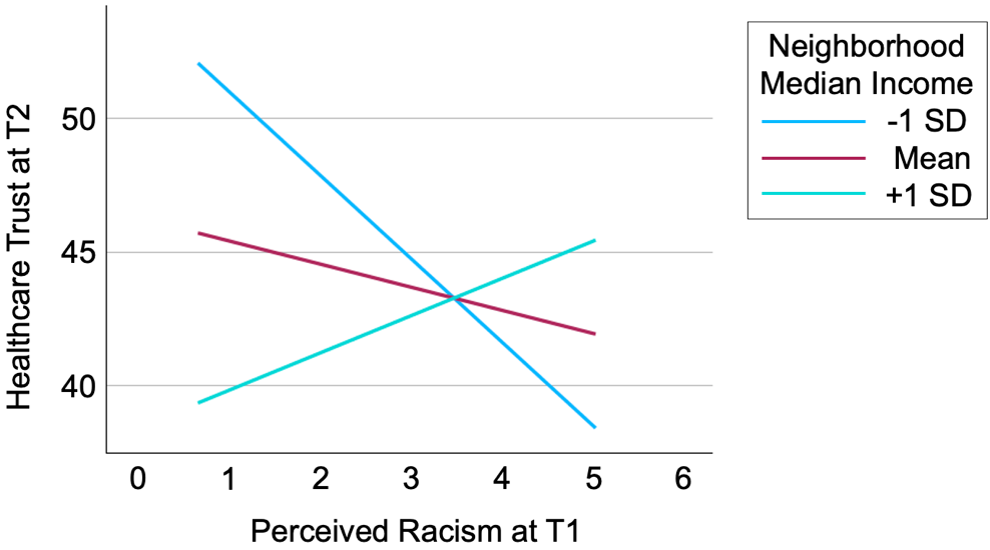 Line graph of the interaction between perceived racism and neighborhood median income predicting healthcare trust. Simple slopes are depicted for AYA 1 SD below the mean neighborhood median income (B = -3.11, p < .001), at the mean neighborhood median income (B = -.86, p = .135), and 1 SD above the mean neighborhood median income (B = 1.39, p = .192).
Line graph of the interaction between perceived racism and neighborhood median income predicting healthcare trust. Simple slopes are depicted for AYA 1 SD below the mean neighborhood median income (B = -3.11, p < .001), at the mean neighborhood median income (B = -.86, p = .135), and 1 SD above the mean neighborhood median income (B = 1.39, p = .192).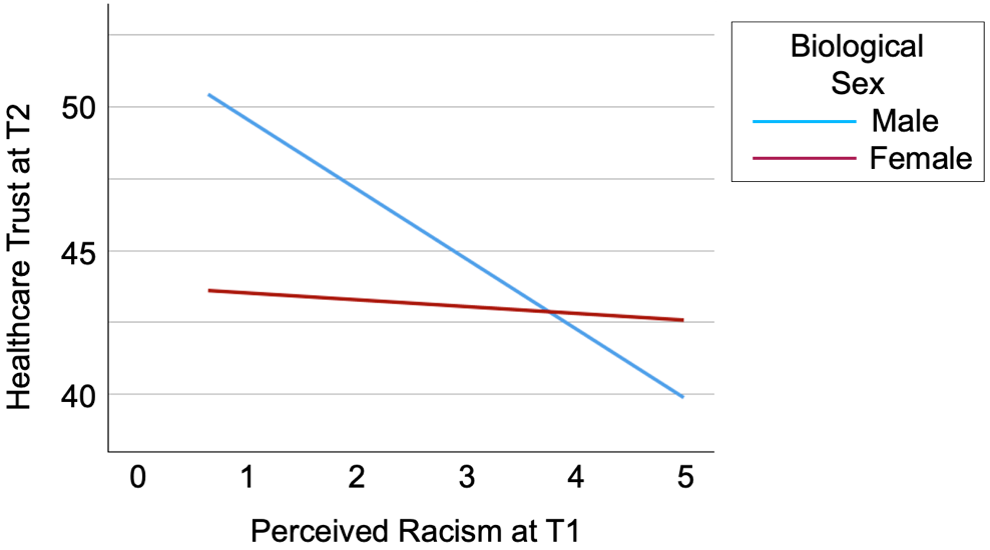 Line graph of the interaction between perceived racism and biological sex predicting healthcare trust. Simple slopes are depicted for male AYA (B = -2.42, p = .002) and female AYA (B = .24, p = .792).
Line graph of the interaction between perceived racism and biological sex predicting healthcare trust. Simple slopes are depicted for male AYA (B = -2.42, p = .002) and female AYA (B = .24, p = .792).