
Neonatal Quality Improvement 5
Session: Neonatal Quality Improvement 5
 Credit")
Nicholas Puoplo, MD (he/him/his)
NICU Fellow
New York Presbyterian- Columbia
Icahn School of Medicine at Mount Sinai Department of Pediatrics
Bronx, New York, United States
.png) Key driver diagram created by multidisciplinary team that identifies the most important interventions necessary to influence our key drivers in order to reach our smart aim.
Key driver diagram created by multidisciplinary team that identifies the most important interventions necessary to influence our key drivers in order to reach our smart aim. .png) Algorithm created to determine which intubations qualify as “controlled” and how to proceed on a patient-by-patient basis. QR code is included for intubation and adverse event tracking. This algorithm can be followed for every neonatal intubation.
Algorithm created to determine which intubations qualify as “controlled” and how to proceed on a patient-by-patient basis. QR code is included for intubation and adverse event tracking. This algorithm can be followed for every neonatal intubation.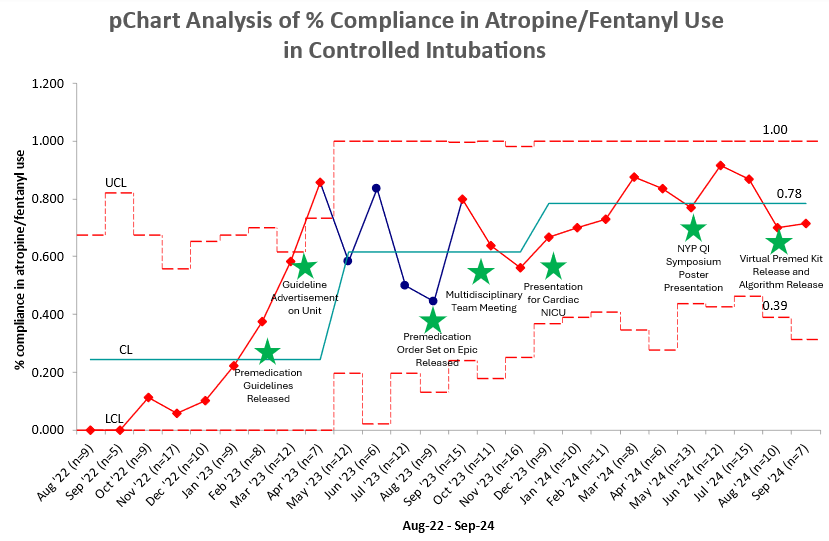 pChart showing monthly % compliance from August 2022 to September 2024 with PDSA cycles noted by stars. An early positive trend is noted from November 2022 to April 2023. A shift that changed our median was noted from December 2023 to July 2024.Key driver diagram created by multidisciplinary team that identifies the most important interventions necessary to influence our key drivers in order to reach our smart aim. Algorithm created to determine which intubations qualify as “controlled” and how to proceed on a patient-by-patient basis. QR code is included for intubation and adverse event tracking. This algorithm can be followed for every neonatal intubation.pChart showing monthly % compliance from August 2022 to September 2024 with PDSA cycles noted by stars. An early positive trend is noted from November 2022 to April 2023. A shift that changed our median was noted from December 2023 to July 2024.
pChart showing monthly % compliance from August 2022 to September 2024 with PDSA cycles noted by stars. An early positive trend is noted from November 2022 to April 2023. A shift that changed our median was noted from December 2023 to July 2024.Key driver diagram created by multidisciplinary team that identifies the most important interventions necessary to influence our key drivers in order to reach our smart aim. Algorithm created to determine which intubations qualify as “controlled” and how to proceed on a patient-by-patient basis. QR code is included for intubation and adverse event tracking. This algorithm can be followed for every neonatal intubation.pChart showing monthly % compliance from August 2022 to September 2024 with PDSA cycles noted by stars. An early positive trend is noted from November 2022 to April 2023. A shift that changed our median was noted from December 2023 to July 2024.