
Quality Improvement/Patient Safety 5
Session: Quality Improvement/Patient Safety 5
 Credit")

Jennifer McKinsey, MD
Clinical Associate Professor of Pediatrics
Children's Mercy Kansas City
Overland Park, Kansas, United States
.jpg) Our primary outcome measure (A) was the percent of patients with penicillin allergy labels seen in the urgent care each month. Our secondary outcome measure (B) was the percent of patients who had their penicillin allergy delabeled. Process measures included (C) the percent of penicillin allergy labels canceled by history alone and (D) the percent of patients with penicillin allergy labels who were referred for subspecialty evaluation to either Allergy or Infectious Disease clinics.
Our primary outcome measure (A) was the percent of patients with penicillin allergy labels seen in the urgent care each month. Our secondary outcome measure (B) was the percent of patients who had their penicillin allergy delabeled. Process measures included (C) the percent of penicillin allergy labels canceled by history alone and (D) the percent of patients with penicillin allergy labels who were referred for subspecialty evaluation to either Allergy or Infectious Disease clinics. 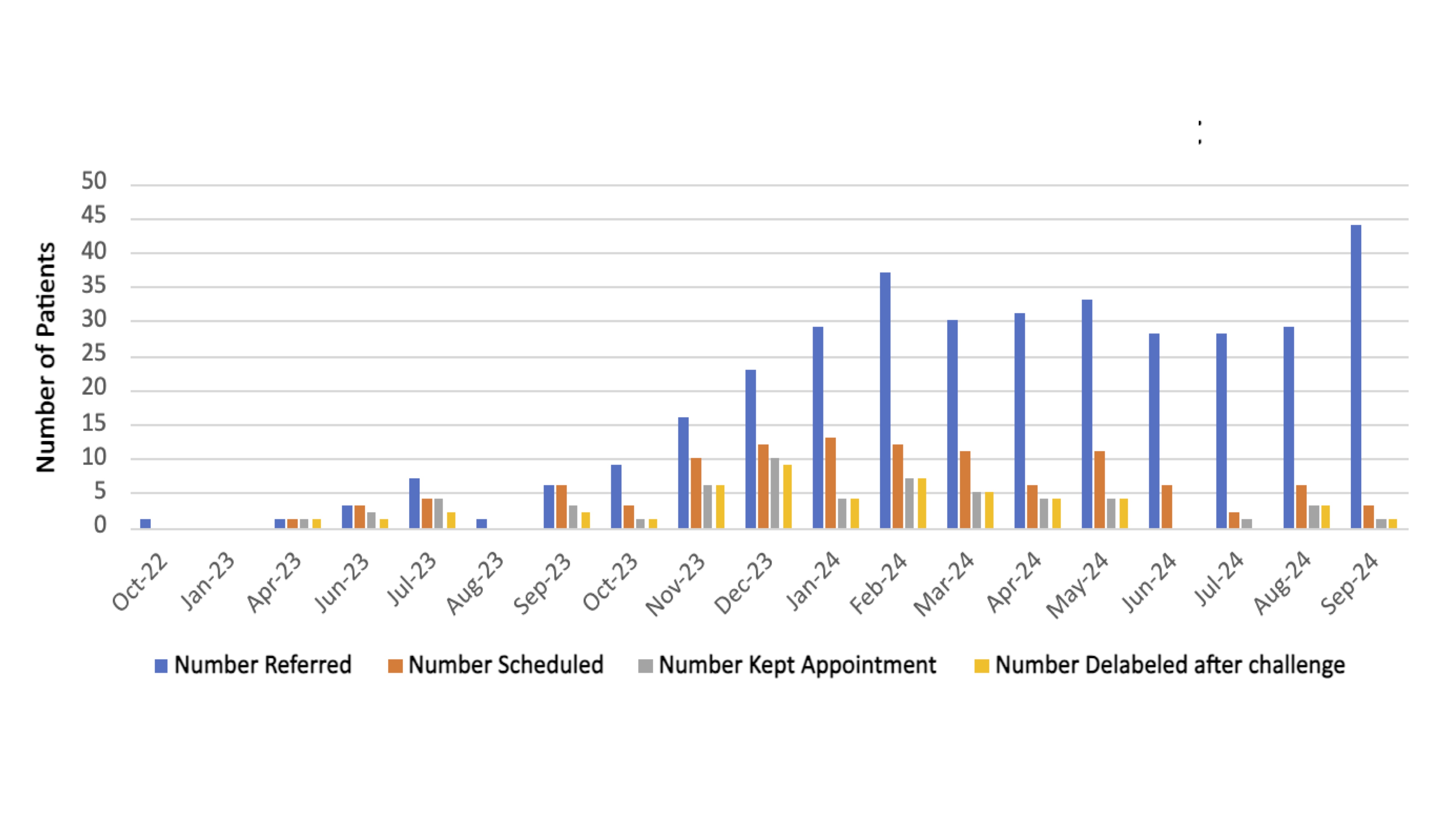 This bar graph illustrates the progressive patient attrition from referral to subspecialty visit with the number of patients referred for penicillin allergy evaluation depicted by the blue bars, the number of patients scheduled for subspecialty appointment depicted by the orange bars, and the number of patients who kept their subspecialty appointment depicted by the gray bars. Many patients could not be reached to schedule their subspecialty appointments. Many patients referred in June 2023 and later have not yet had their subspecialty appointments scheduled or been evaluated due to the 4-5 month delay between referral and subspecialty visit.
This bar graph illustrates the progressive patient attrition from referral to subspecialty visit with the number of patients referred for penicillin allergy evaluation depicted by the blue bars, the number of patients scheduled for subspecialty appointment depicted by the orange bars, and the number of patients who kept their subspecialty appointment depicted by the gray bars. Many patients could not be reached to schedule their subspecialty appointments. Many patients referred in June 2023 and later have not yet had their subspecialty appointments scheduled or been evaluated due to the 4-5 month delay between referral and subspecialty visit.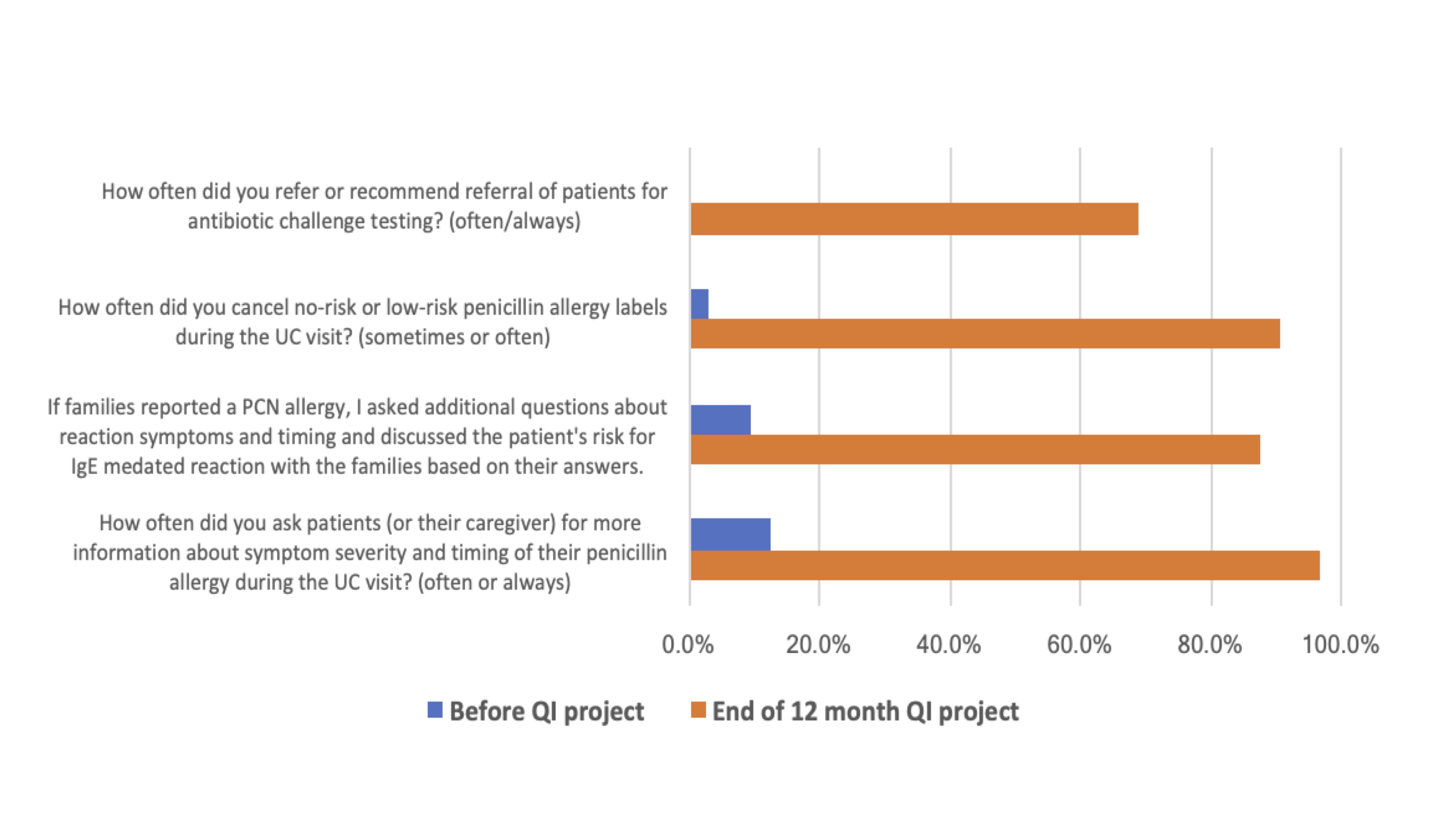 Nurse and clinician survey responses on their approach to evaluating penicillin allergy labels before and after the quality improvement project.
Nurse and clinician survey responses on their approach to evaluating penicillin allergy labels before and after the quality improvement project.