
Clinical Bioethics
Session: Clinical Bioethics
Nithya Sivakumar, BA, MBE (she/her/hers)
Medical Student
University of California, Davis, School of Medicine
Sacramento, California, United States
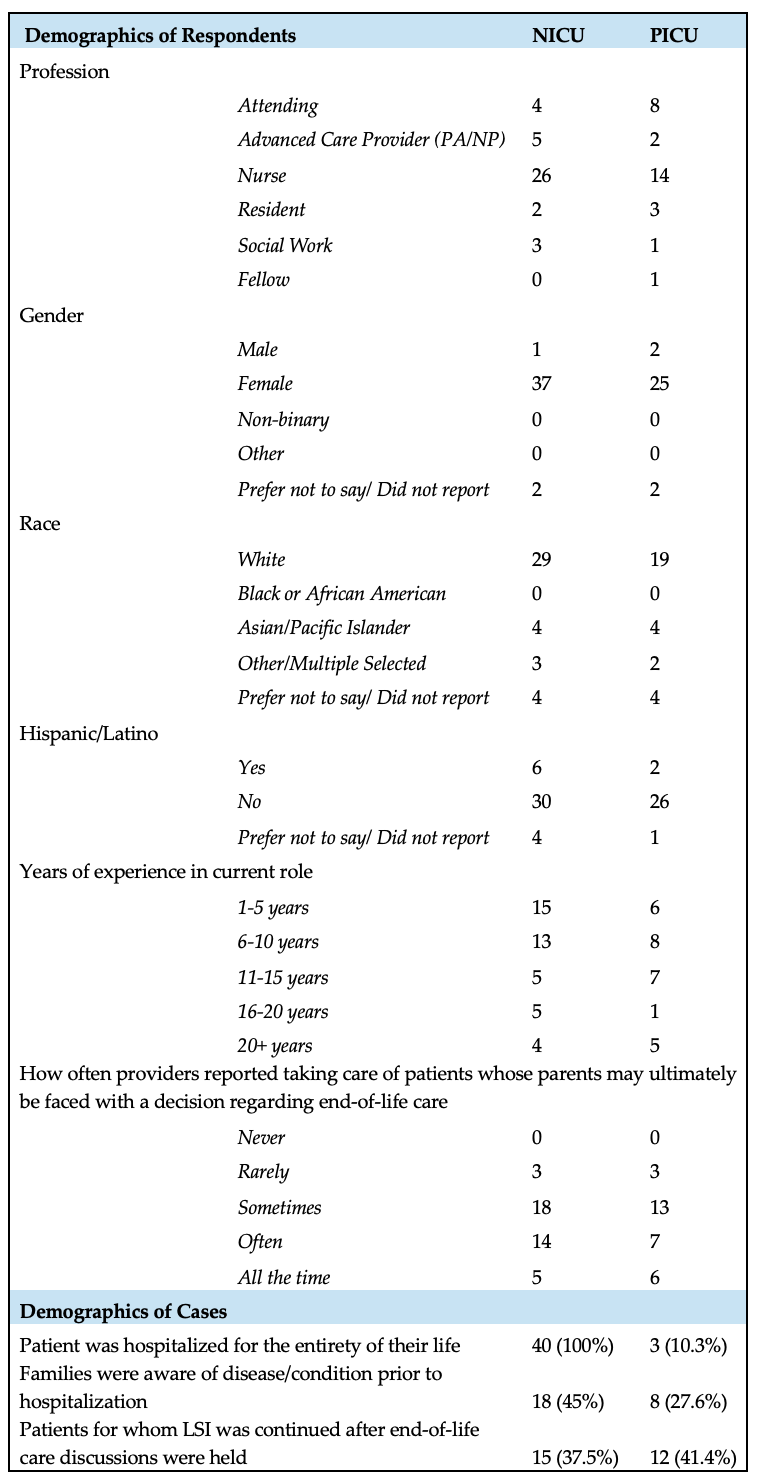 Demographic information for respondents and cases. There were 40 responses from providers in the NICU, and 29 from providers in the PICU.
Demographic information for respondents and cases. There were 40 responses from providers in the NICU, and 29 from providers in the PICU. 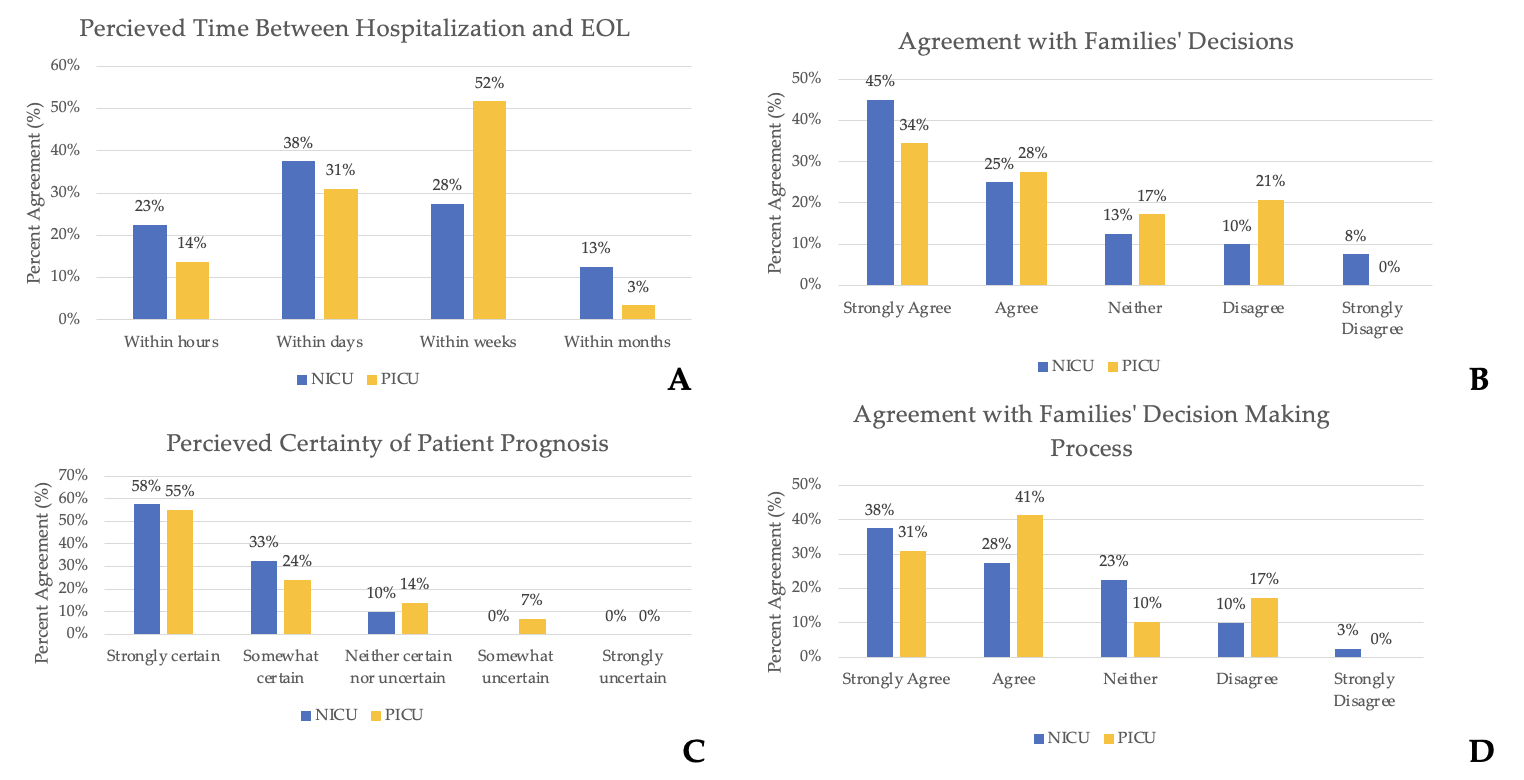 (A) Bar chart depicting perceived time between hospitalization and end of life (EOL) care discussions. (B) Bar chart depicting provider agreement with families’ decision regarding continuing or withdrawing life sustaining therapy after end-of-life care discussions. (C) Bar chart depicting perceived certainty of patient prognosis at the time of end-of-life care discussions. (D) Bar chart depicting provider agreement with how families came to the decision regarding whether to continue or withdraw life sustaining therapies after end-of-life care discussions.
(A) Bar chart depicting perceived time between hospitalization and end of life (EOL) care discussions. (B) Bar chart depicting provider agreement with families’ decision regarding continuing or withdrawing life sustaining therapy after end-of-life care discussions. (C) Bar chart depicting perceived certainty of patient prognosis at the time of end-of-life care discussions. (D) Bar chart depicting provider agreement with how families came to the decision regarding whether to continue or withdraw life sustaining therapies after end-of-life care discussions.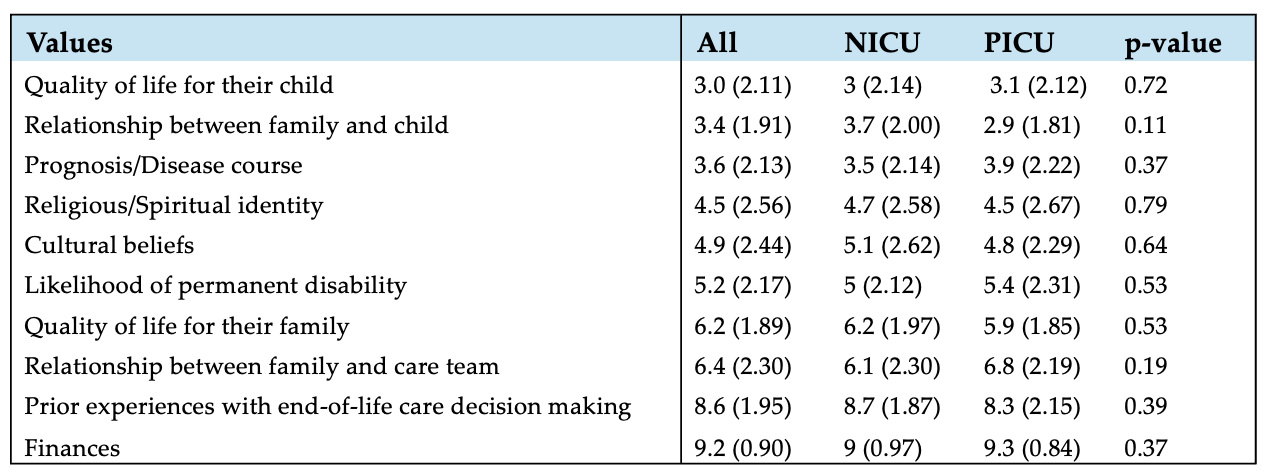 Results on ranking question of the research survey. Respondents were asked to rank values that their family considered from most (1) to least (10) important, reported as mean (standard deviation).
Results on ranking question of the research survey. Respondents were asked to rank values that their family considered from most (1) to least (10) important, reported as mean (standard deviation). 