
Neonatal Quality Improvement 5
Session: Neonatal Quality Improvement 5

Ernest Lai, MD
Neonatology Fellow
CHOC Children's Hospital of Orange County / University of California, Irvine, School of Medicine
Santa Ana, California, United States
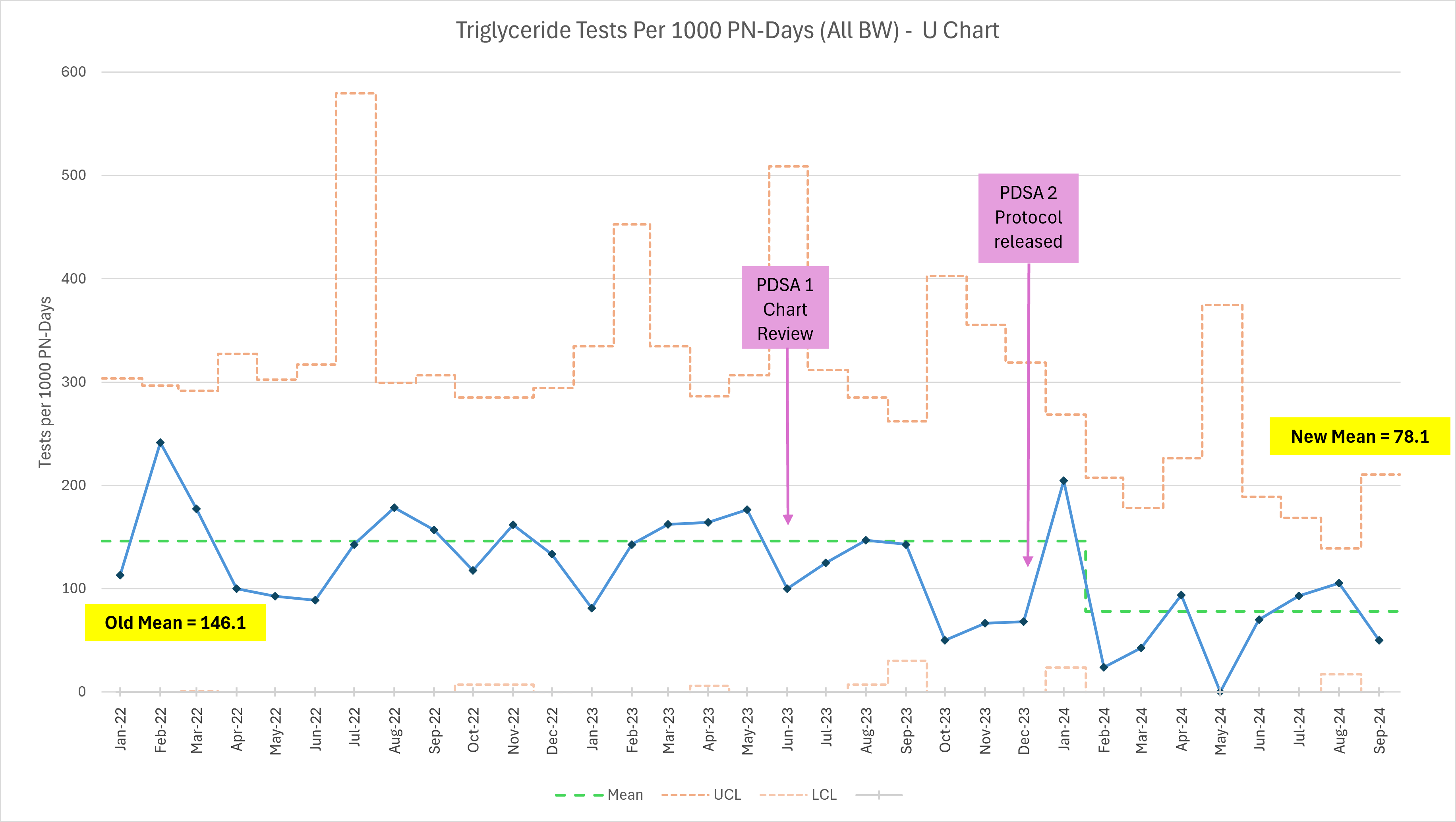 Primary outcome measure – annotated U chart depicting the number of triglyceride tests per 1000 parental nutrition days by month in all infants with BW ≤ 1500g from January 2022 through September 2024. UCL, upper control limit; LCL, lower control limit.
Primary outcome measure – annotated U chart depicting the number of triglyceride tests per 1000 parental nutrition days by month in all infants with BW ≤ 1500g from January 2022 through September 2024. UCL, upper control limit; LCL, lower control limit.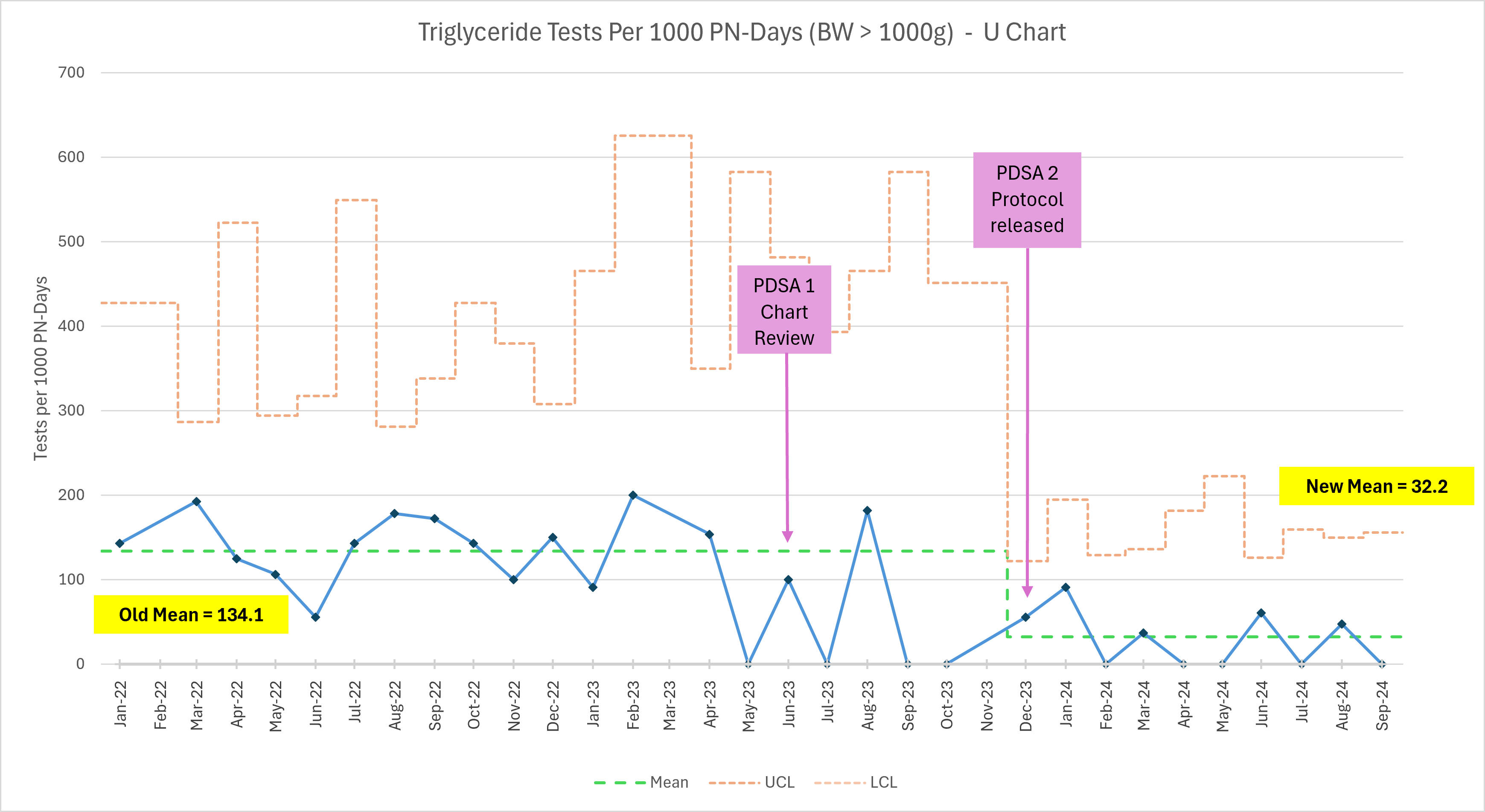 Secondary outcome measure – annotated U chart depicting the number of triglyceride tests per 1000 parental nutrition days by month in infants with BW > 1000g from January 2022 through September 2024. UCL, upper control limit; LCL, lower control limit.
Secondary outcome measure – annotated U chart depicting the number of triglyceride tests per 1000 parental nutrition days by month in infants with BW > 1000g from January 2022 through September 2024. UCL, upper control limit; LCL, lower control limit.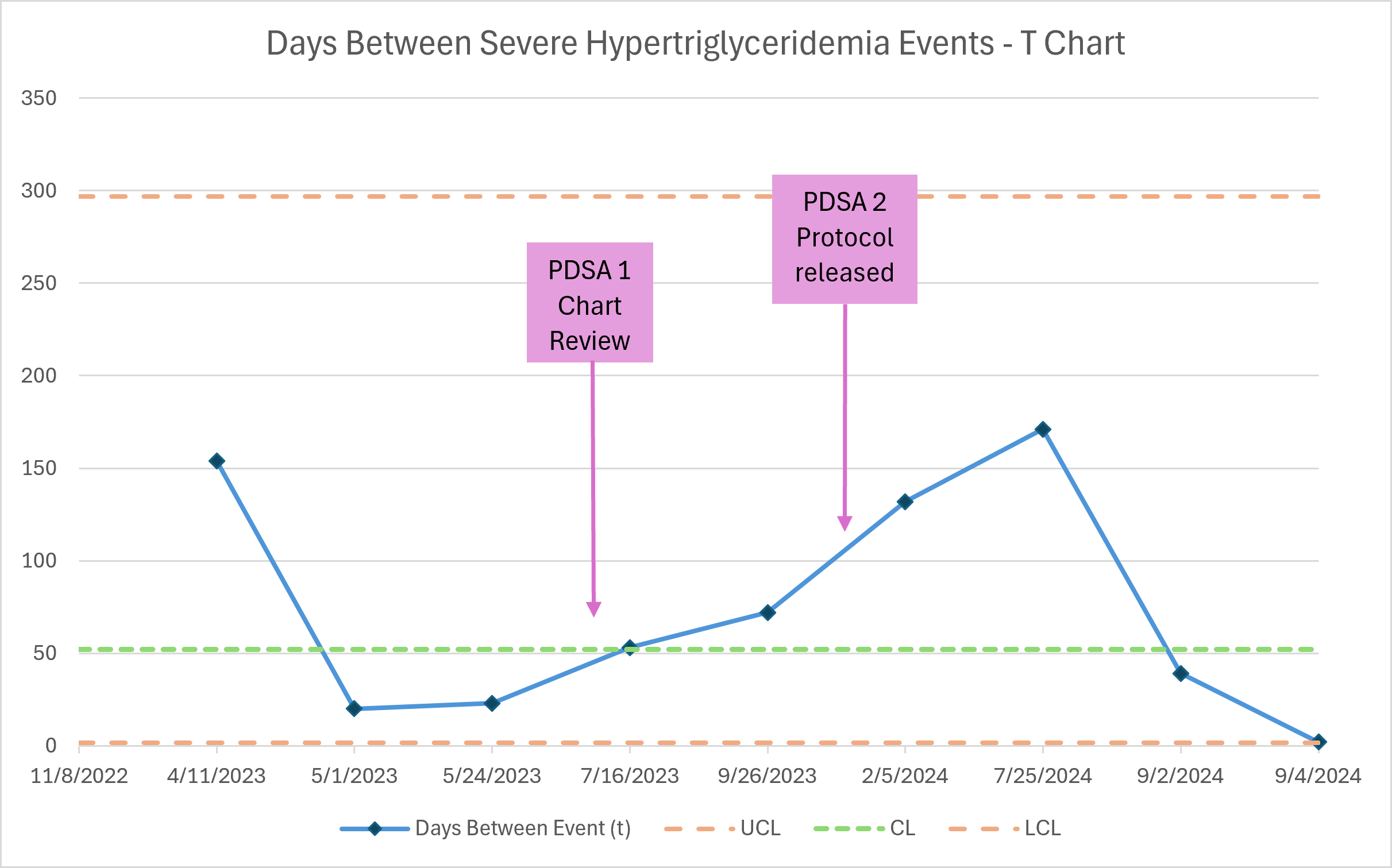 Balancing measure – annotated T chart depicting days between severe hypertriglyceridemia events (defined as a serum TG > 500 mg/dL) in all infants with BW ≤ 1500g from January 2022 through September 2024. UCL, upper control limit; LCL, lower control limit; CL, center line.
Balancing measure – annotated T chart depicting days between severe hypertriglyceridemia events (defined as a serum TG > 500 mg/dL) in all infants with BW ≤ 1500g from January 2022 through September 2024. UCL, upper control limit; LCL, lower control limit; CL, center line. 