
Technology 2: Telemedicine
Session: Technology 2: Telemedicine
.jpg "Seethal A. Jacob, MD, MS (she/her/hers) photo")
Seethal A. Jacob, MD, MS (she/her/hers)
Associate Professor of Pediatrics
Indiana University School of Medicine
Indianapolis, Indiana, United States
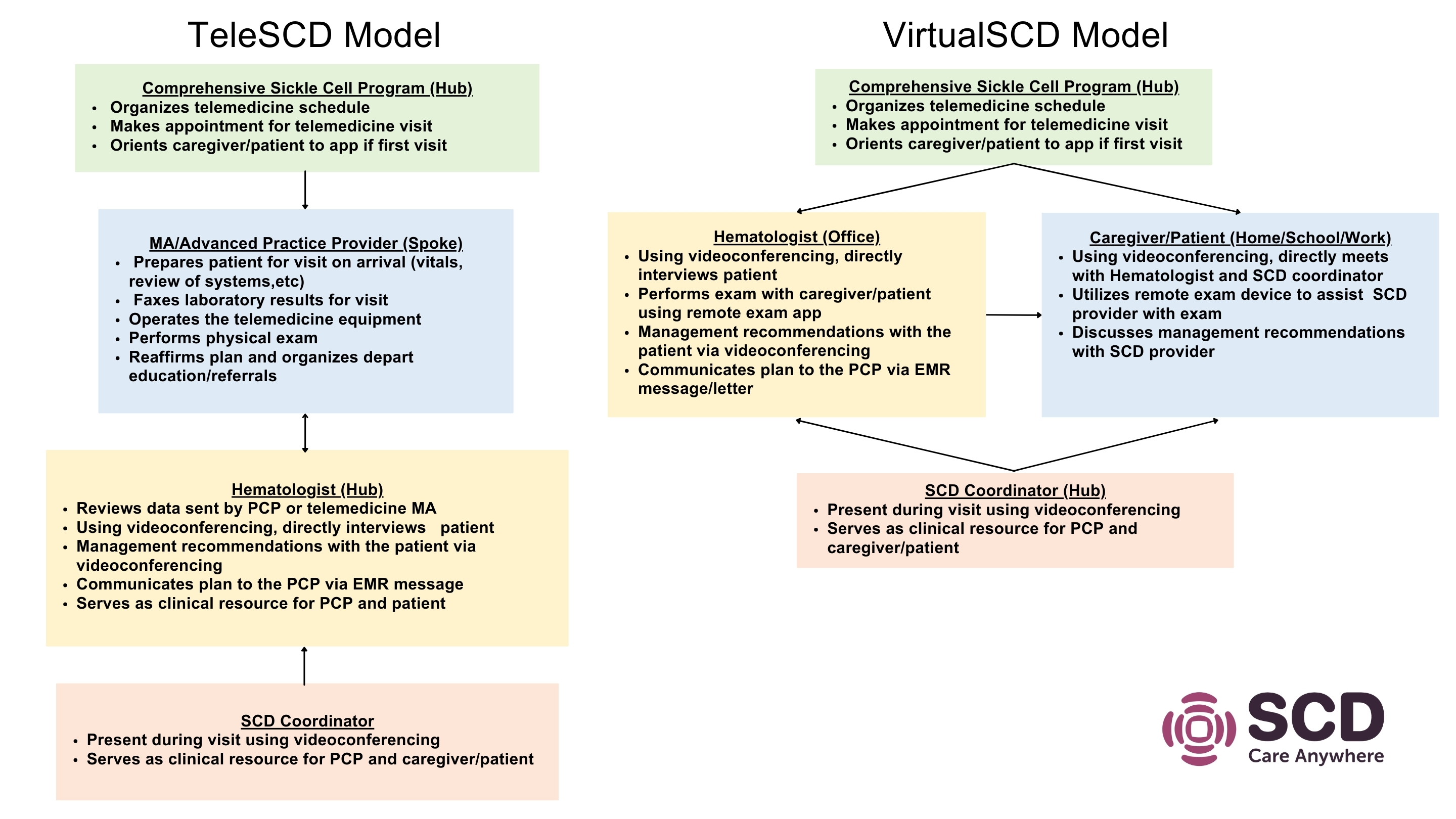 Hub-and-Spoke and Direct-to-Consumer models developed and adapted with caregiver and patient input on barriers and facilitators to telemedicine use.
Hub-and-Spoke and Direct-to-Consumer models developed and adapted with caregiver and patient input on barriers and facilitators to telemedicine use.