
Developmental and Behavioral Pediatrics 4: ADHD
Session: Developmental and Behavioral Pediatrics 4: ADHD
 photo")
Samuel D. Pimentel, PhD (he/him/his)
Assistant Professor of Statistics
University of California Berkeley
Berkeley, California, United States
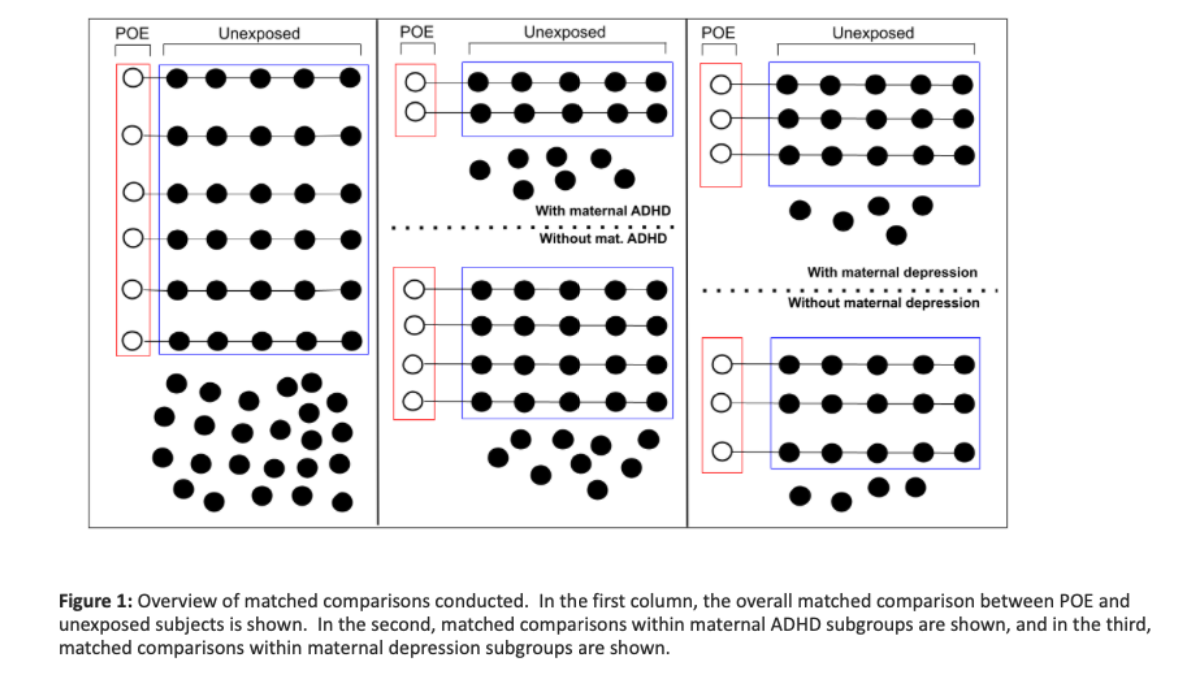 In the first column, the overall matched comparison between POE and unexposed subjects is shown. In the second, matched comparisons within maternal ADHD subgroups are shown, and in the third, matched comparisons within maternal depression subgroups are shown.
In the first column, the overall matched comparison between POE and unexposed subjects is shown. In the second, matched comparisons within maternal ADHD subgroups are shown, and in the third, matched comparisons within maternal depression subgroups are shown. 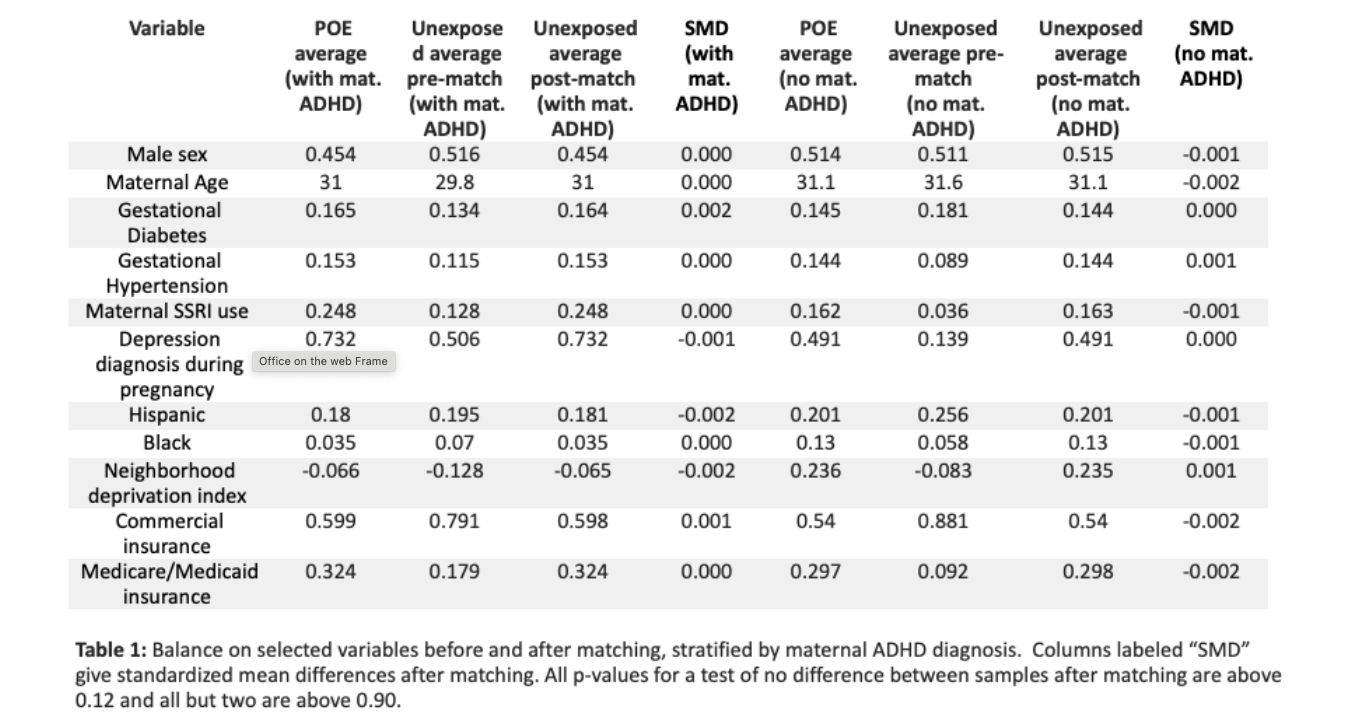 Columns labeled “SMD” give standardized mean differences after matching. All p-values for a test of no difference between samples after matching are above 0.12 and all but two are above 0.90.
Columns labeled “SMD” give standardized mean differences after matching. All p-values for a test of no difference between samples after matching are above 0.12 and all but two are above 0.90. 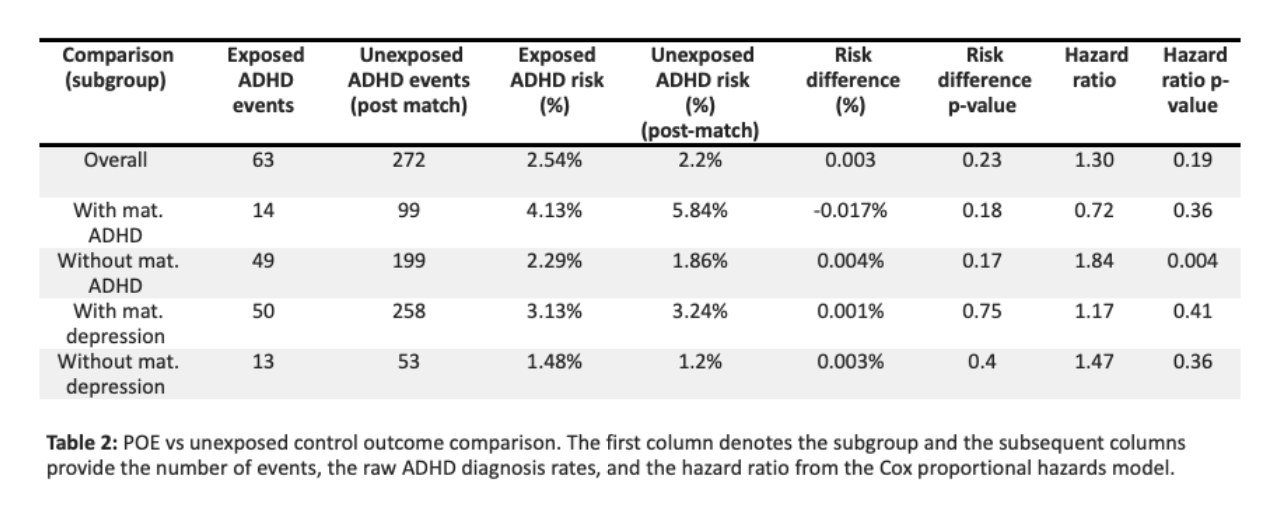 The first column denotes the subgroup and the subsequent columns provide the number of events, the raw ADHD diagnosis rates, and the hazard ratio from the Cox proportional hazards model.
The first column denotes the subgroup and the subsequent columns provide the number of events, the raw ADHD diagnosis rates, and the hazard ratio from the Cox proportional hazards model. 