
Neonatal Fetal Nutrition & Metabolism 2
Session: Neonatal Fetal Nutrition & Metabolism 2
 photo")
Anjali Borsum, BS (she/her/hers)
Medical Student
Medical University of South Carolina College of Medicine
Charleston, South Carolina, United States
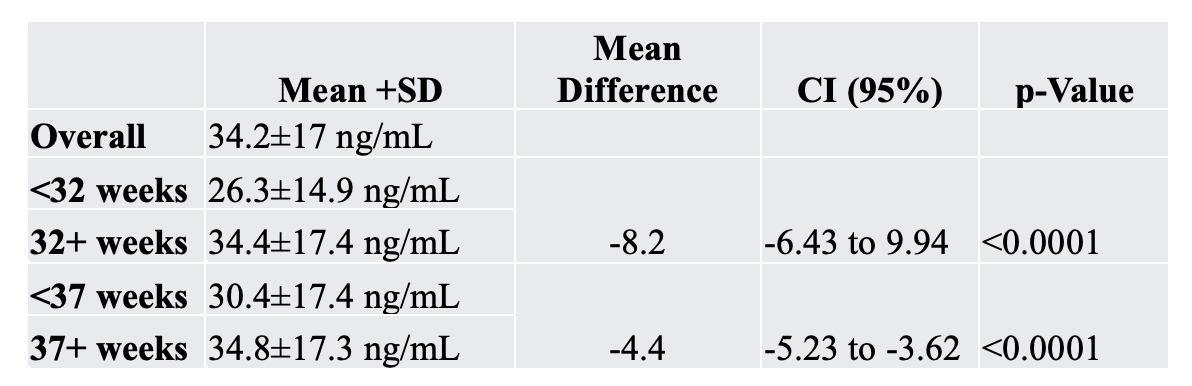 The overall mean ± SD 25(OH)D concentration was 34.2±17 ng/mL. Mothers delivering <37 weeks had significantly lower 25(OH)D (30.4±17.4 ng/mL) compared to those delivering at ≥37 wks (34.8±17.3 ng/mL), with a mean difference of -4.4 ng/mL (95% CI: -5.23 to -3.62, p<0.0001). This difference was accentuated among mothers delivering < 32 weeks (26.3±14.9 ng/mL) compared to those delivering at ≥32 weeks (34.4±17.4 ng/mL), with a mean difference of 8.2 ng/mL (95% CI: 6.43 to 9.94, p<0.0001).
The overall mean ± SD 25(OH)D concentration was 34.2±17 ng/mL. Mothers delivering <37 weeks had significantly lower 25(OH)D (30.4±17.4 ng/mL) compared to those delivering at ≥37 wks (34.8±17.3 ng/mL), with a mean difference of -4.4 ng/mL (95% CI: -5.23 to -3.62, p<0.0001). This difference was accentuated among mothers delivering < 32 weeks (26.3±14.9 ng/mL) compared to those delivering at ≥32 weeks (34.4±17.4 ng/mL), with a mean difference of 8.2 ng/mL (95% CI: 6.43 to 9.94, p<0.0001). 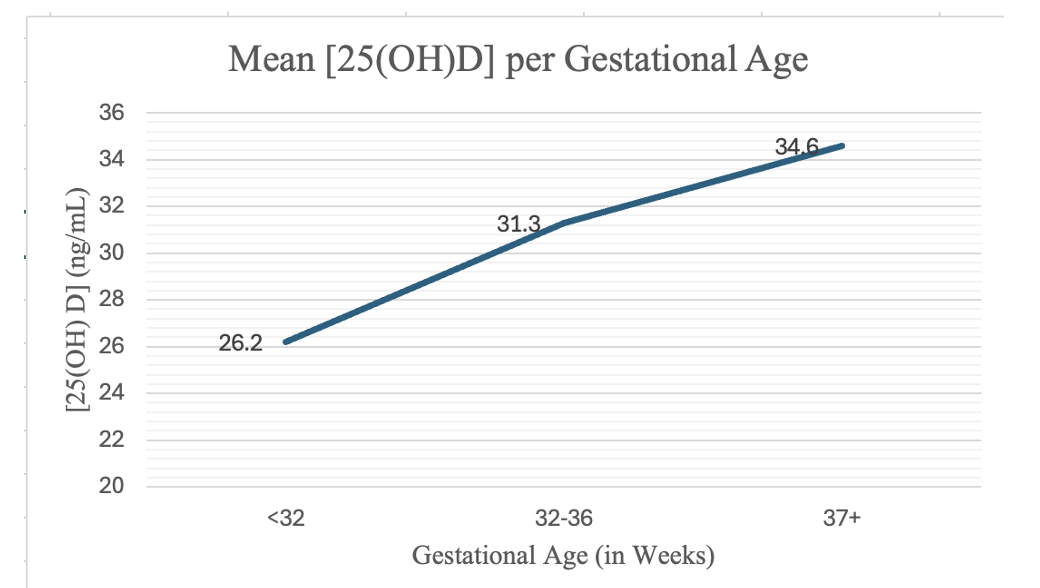 Mothers delivering <37 weeks had significantly lower 25(OH)D concentrations compared to those delivering ≥37 weeks, and the difference was greater for women delivering <32 weeks compared to those delivering at ≥32 weeks.
Mothers delivering <37 weeks had significantly lower 25(OH)D concentrations compared to those delivering ≥37 weeks, and the difference was greater for women delivering <32 weeks compared to those delivering at ≥32 weeks. 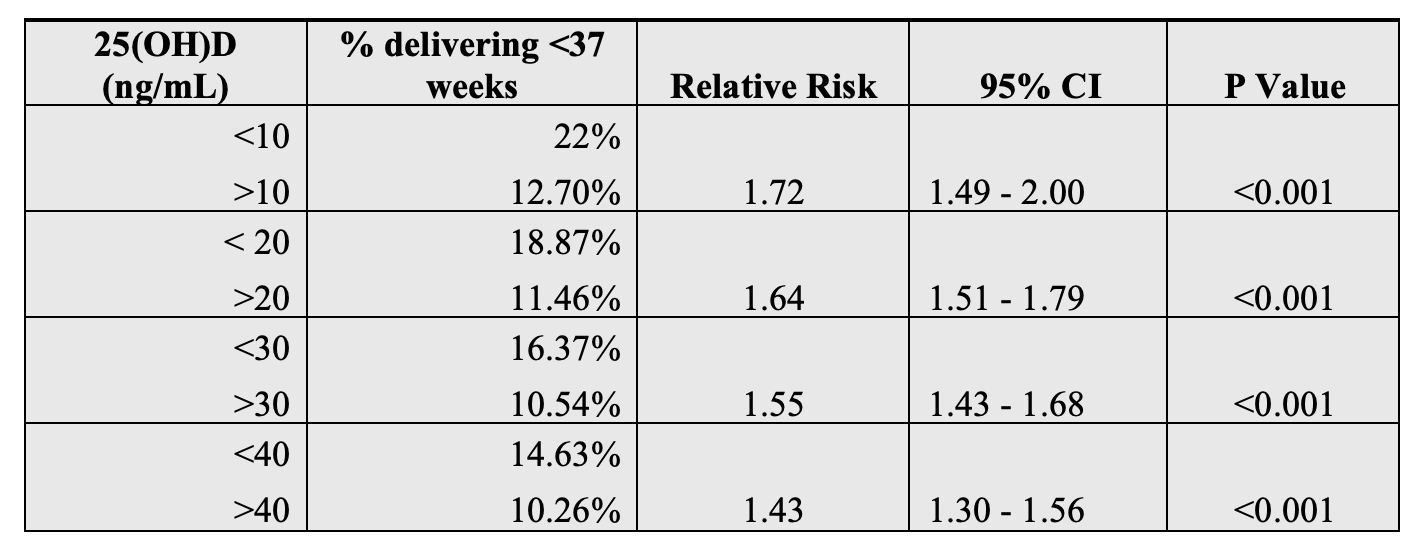 As 25(OH)D levels decrease, the risk of preterm delivery increases. Mothers with severe vitD deficiency ( <10 ng/mL) are 1.72 times more likely to deliver preterm than mothers with 25(OH)D higher than 10 ng/mL. The overall mean ± SD 25(OH)D concentration was 34.2±17 ng/mL. Mothers delivering <37 weeks had significantly lower 25(OH)D (30.4±17.4 ng/mL) compared to those delivering at ≥37 wks (34.8±17.3 ng/mL), with a mean difference of -4.4 ng/mL (95% CI: -5.23 to -3.62, p<0.0001). This difference was accentuated among mothers delivering < 32 weeks (26.3±14.9 ng/mL) compared to those delivering at ≥32 weeks (34.4±17.4 ng/mL), with a mean difference of 8.2 ng/mL (95% CI: 6.43 to 9.94, p<0.0001). Mothers delivering <37 weeks had significantly lower 25(OH)D concentrations compared to those delivering ≥37 weeks, and the difference was greater for women delivering <32 weeks compared to those delivering at ≥32 weeks. As 25(OH)D levels decrease, the risk of preterm delivery increases. Mothers with severe vitD deficiency ( <10 ng/mL) are 1.72 times more likely to deliver preterm than mothers with 25(OH)D higher than 10 ng/mL.
As 25(OH)D levels decrease, the risk of preterm delivery increases. Mothers with severe vitD deficiency ( <10 ng/mL) are 1.72 times more likely to deliver preterm than mothers with 25(OH)D higher than 10 ng/mL. The overall mean ± SD 25(OH)D concentration was 34.2±17 ng/mL. Mothers delivering <37 weeks had significantly lower 25(OH)D (30.4±17.4 ng/mL) compared to those delivering at ≥37 wks (34.8±17.3 ng/mL), with a mean difference of -4.4 ng/mL (95% CI: -5.23 to -3.62, p<0.0001). This difference was accentuated among mothers delivering < 32 weeks (26.3±14.9 ng/mL) compared to those delivering at ≥32 weeks (34.4±17.4 ng/mL), with a mean difference of 8.2 ng/mL (95% CI: 6.43 to 9.94, p<0.0001). Mothers delivering <37 weeks had significantly lower 25(OH)D concentrations compared to those delivering ≥37 weeks, and the difference was greater for women delivering <32 weeks compared to those delivering at ≥32 weeks. As 25(OH)D levels decrease, the risk of preterm delivery increases. Mothers with severe vitD deficiency ( <10 ng/mL) are 1.72 times more likely to deliver preterm than mothers with 25(OH)D higher than 10 ng/mL. 