
Emergency Medicine 5
Session: Emergency Medicine 5
 Credit")
 photo")
Justin J. Assioun, MD (he/him/his)
Pediatric Emergency Fellow
University of California, San Diego School of Medicine
La Jolls, California, United States
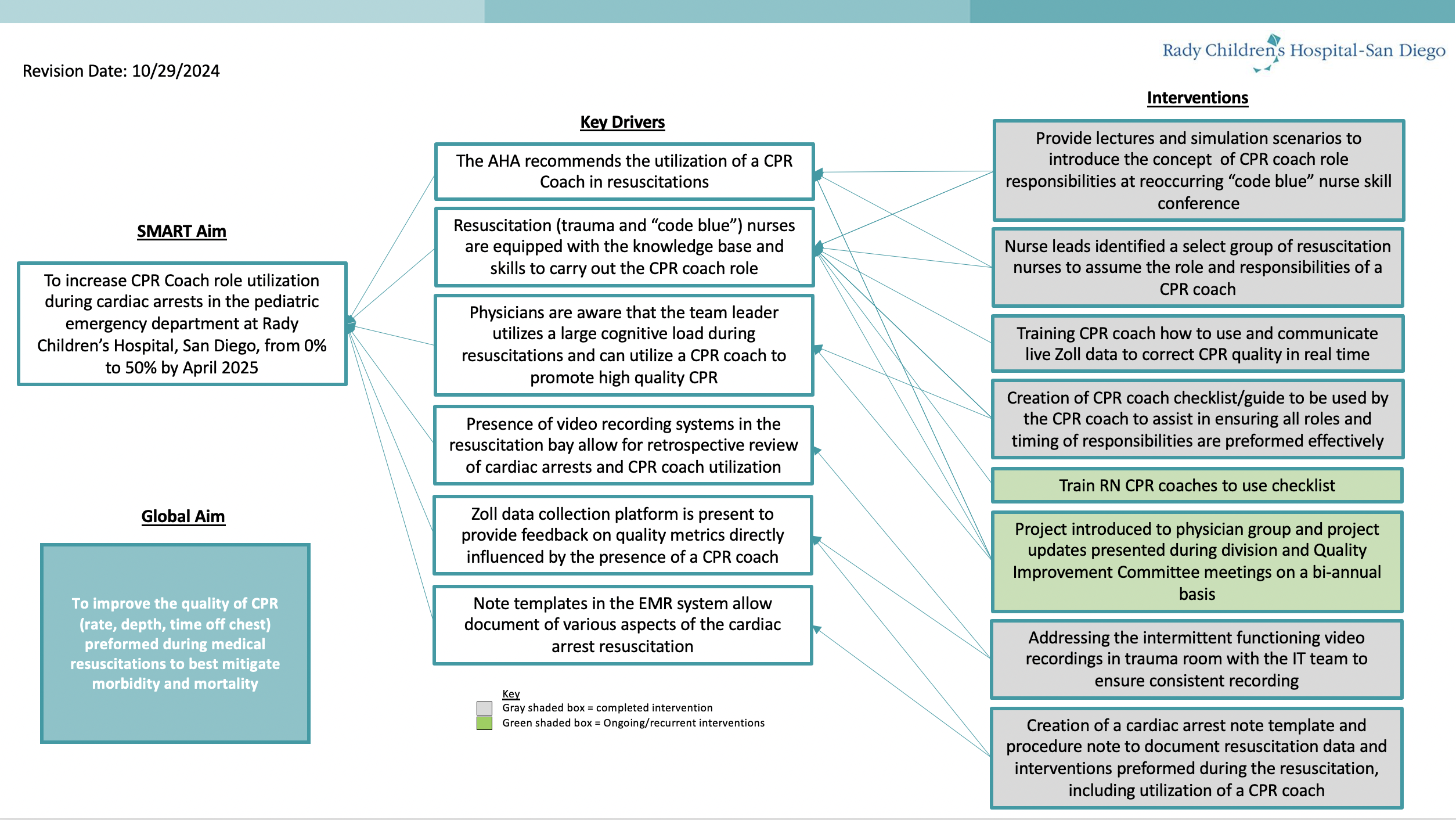 Key Driver Diagram
Key Driver Diagram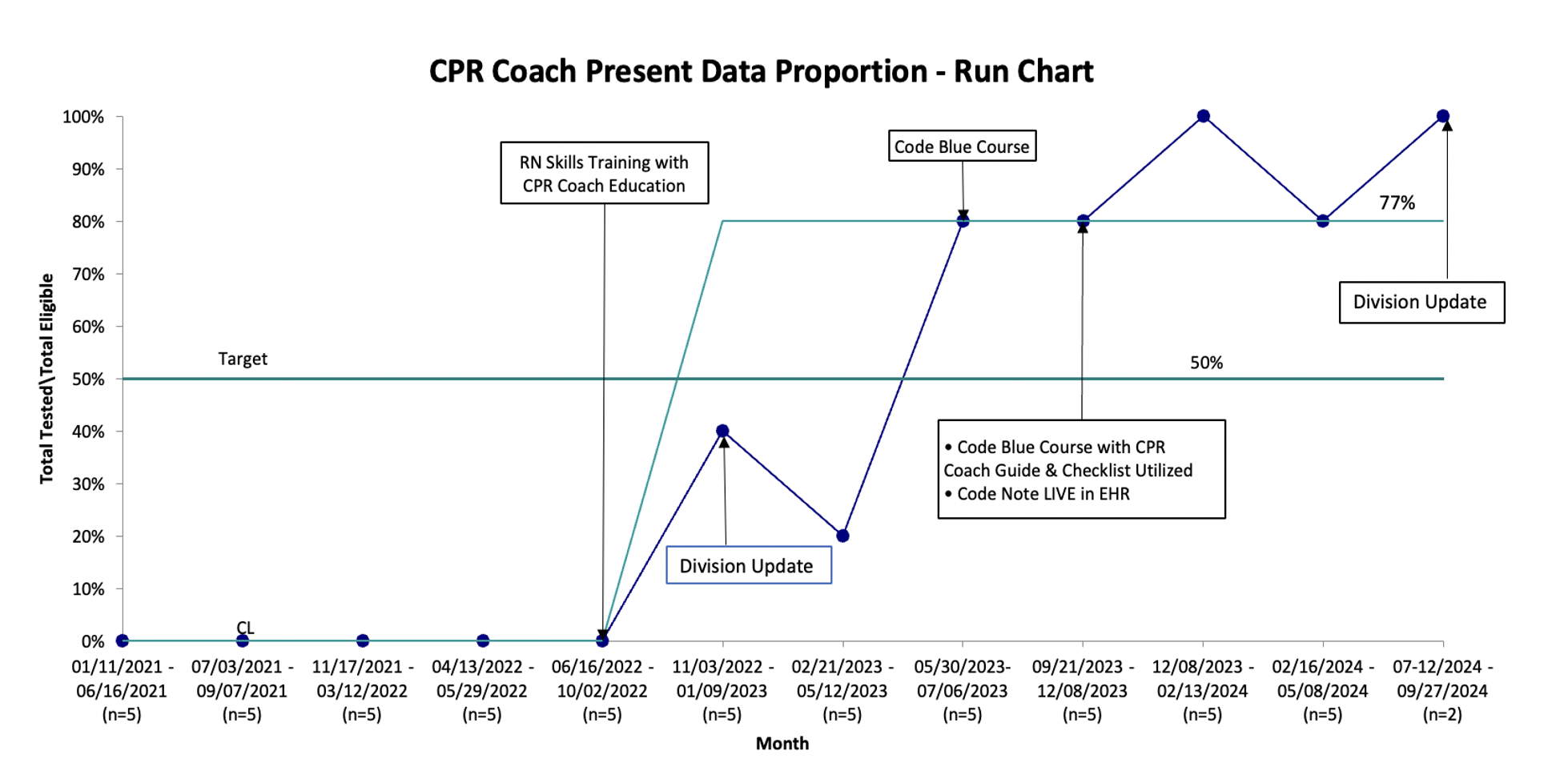 CPR Coach Present Run Chart
CPR Coach Present Run Chart 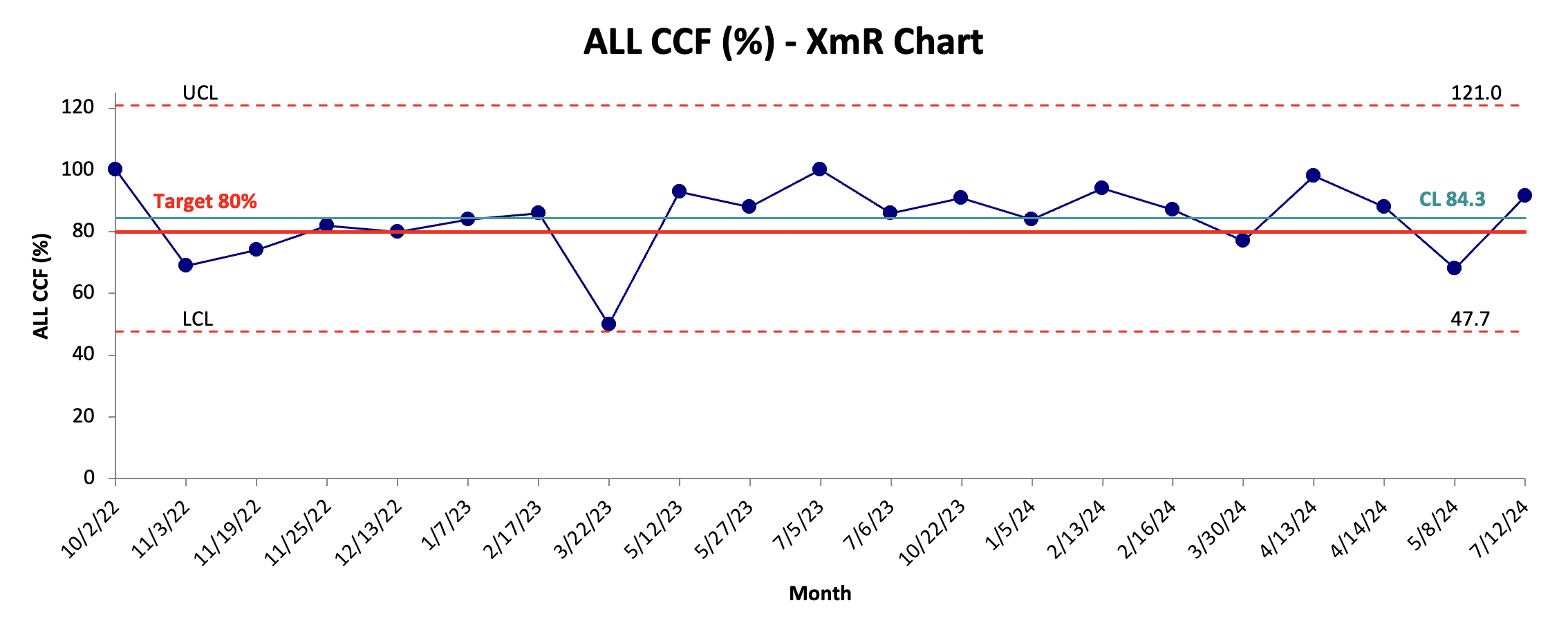 CCF% XmR Chart
CCF% XmR Chart 