
Quality Improvement/Patient Safety 6
Session: Quality Improvement/Patient Safety 6
 Credit")
Lece Webb, MD
Assistant Professor
University of Alabama School of Medicine
Birmingham, Alabama, United States
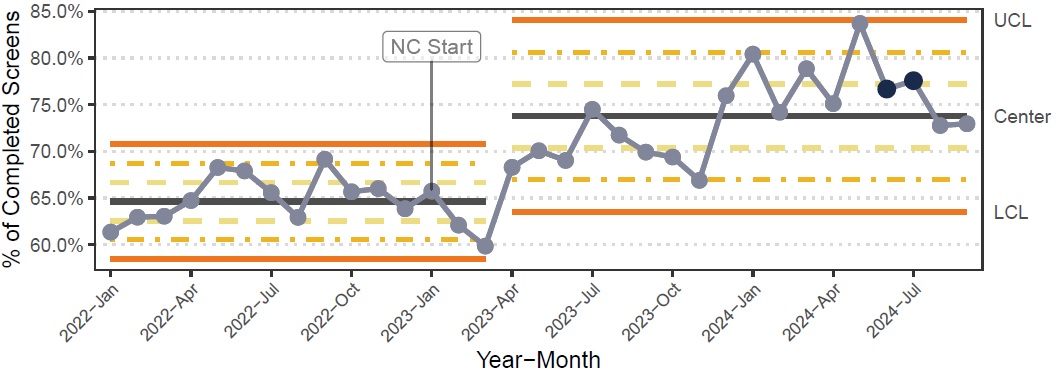 The annotation “NC Starts” at January 2024 shows the beginning of the nutrition collaborative for the five original units. The baseline comprises the period January 2022 to March 2023. Centerline (CL) changes were implemented through Nelson’s rule (Reynolds et al, 2021) when nine or more points fall above/below a CL.
The annotation “NC Starts” at January 2024 shows the beginning of the nutrition collaborative for the five original units. The baseline comprises the period January 2022 to March 2023. Centerline (CL) changes were implemented through Nelson’s rule (Reynolds et al, 2021) when nine or more points fall above/below a CL.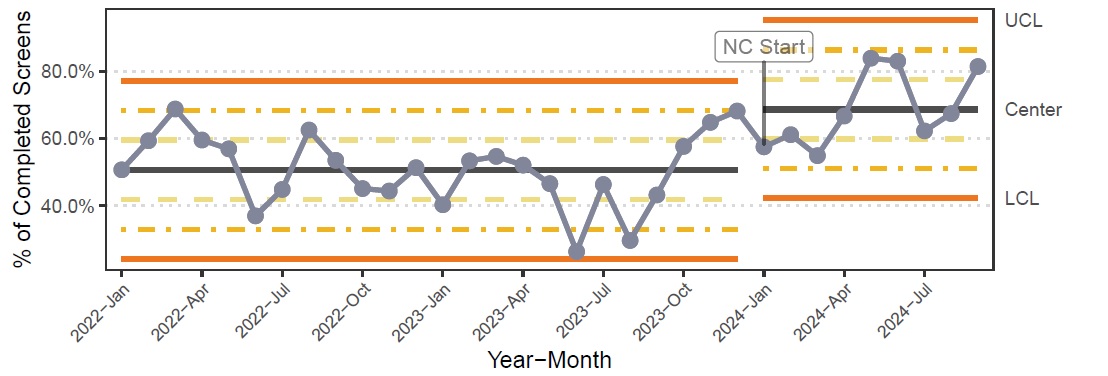 While the sixth unit started nutrition data collection as early as January 2022, its inclusion into the collaborative started on January 2024. This has been captured in the plot with the annotation “NC Starts”. Centerline changes were implemented though Nelson’s rules (Reynolds et al, 2021).
While the sixth unit started nutrition data collection as early as January 2022, its inclusion into the collaborative started on January 2024. This has been captured in the plot with the annotation “NC Starts”. Centerline changes were implemented though Nelson’s rules (Reynolds et al, 2021).