
Neonatal Fetal Nutrition & Metabolism 1
Session: Neonatal Fetal Nutrition & Metabolism 1
Dimitrios Angelis, MD
Neonatologist
University of Texas Southwestern Medical School
Dallas, Texas, United States
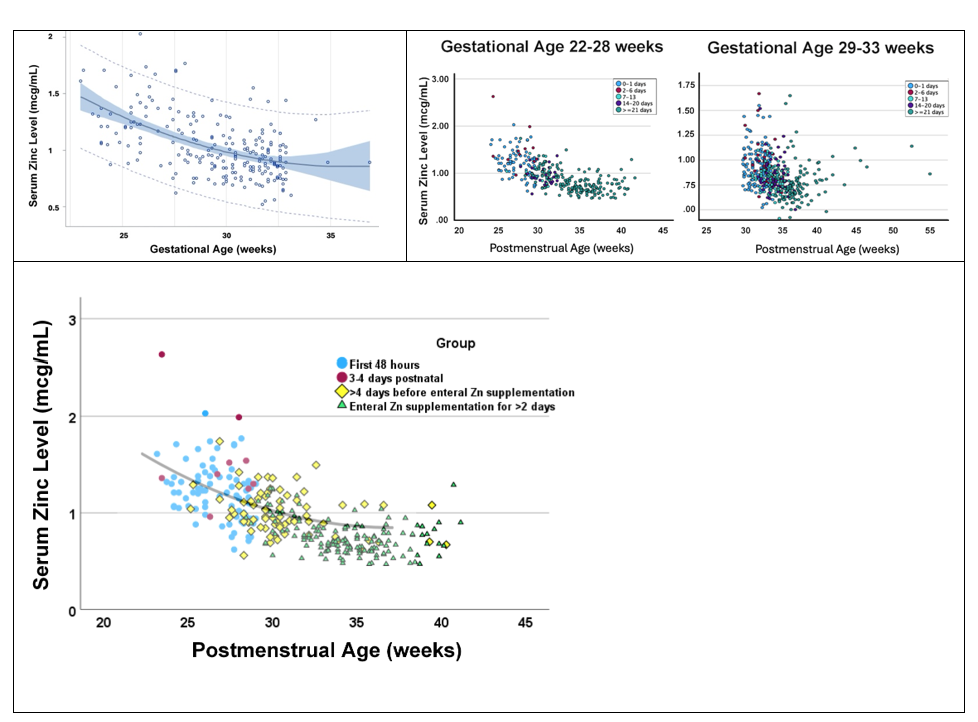 Figure 1a. Early Zinc levels (first 48 hours of life) by gestational age. 95% confidence and prediction intervals of first zinc concentration during the first 48 hours of life versus gestational age among infants <33 weeks gestational age or <1500 g birth weight, excluding those without congenital anomalies or comfort care only. Quadratic regression analysis. Adjusted R2=0.2921, n=228, P<0.0001. Equation: Zn = 5.63727 -0.26622 X GA +0.00370 x GA2. Abbreviations: Zn, serum zinc level; GA, gestational age (weeks)
Figure 1a. Early Zinc levels (first 48 hours of life) by gestational age. 95% confidence and prediction intervals of first zinc concentration during the first 48 hours of life versus gestational age among infants <33 weeks gestational age or <1500 g birth weight, excluding those without congenital anomalies or comfort care only. Quadratic regression analysis. Adjusted R2=0.2921, n=228, P<0.0001. Equation: Zn = 5.63727 -0.26622 X GA +0.00370 x GA2. Abbreviations: Zn, serum zinc level; GA, gestational age (weeks)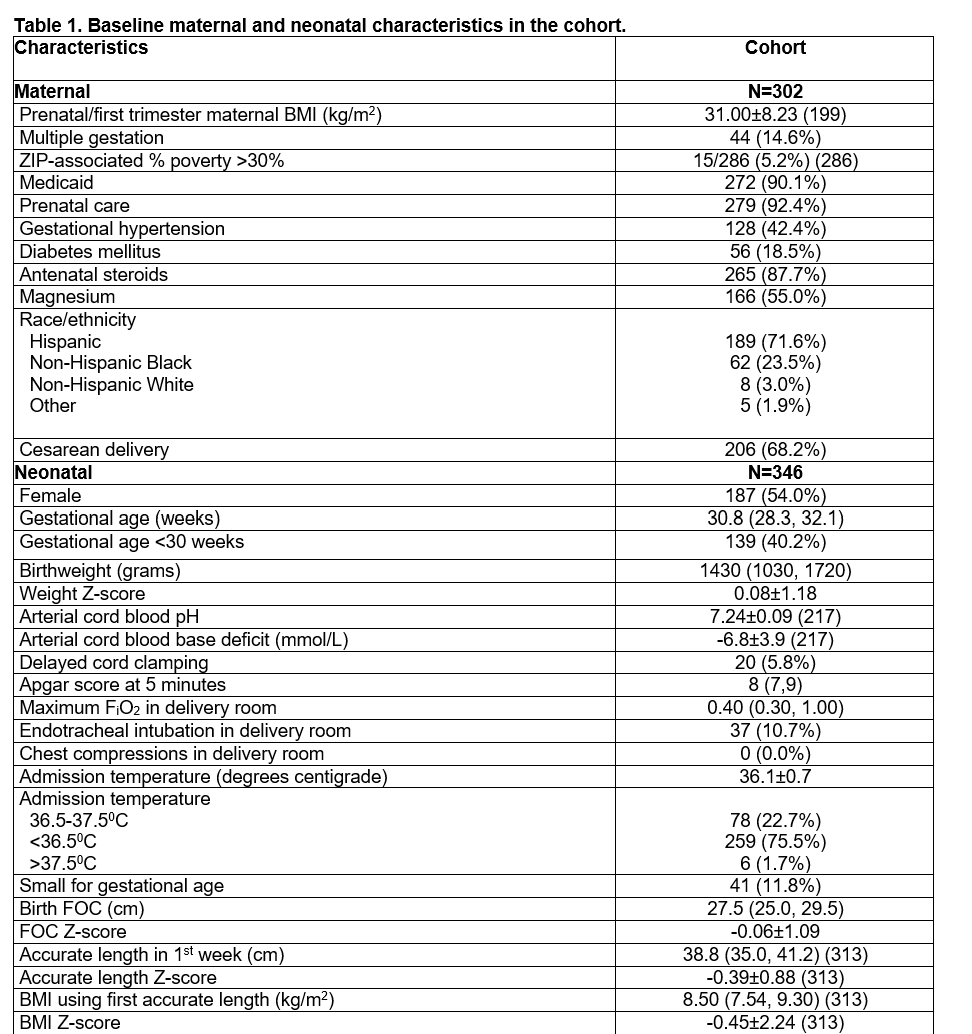 The discrepancy between the number of maternal and neonatal characteristics corresponds to multiple pregnancies.
The discrepancy between the number of maternal and neonatal characteristics corresponds to multiple pregnancies. Mixed model generalized linear equation by rank, 768 measurements among 352 neonates
Mixed model generalized linear equation by rank, 768 measurements among 352 neonates