
Neonatal GI Physiology & NEC 1
Session: Neonatal GI Physiology & NEC 1
 photo")
Alain Cuna, MD (he/him/his)
Neonatologist
Children's Mercy Hospitals and Clinics
University of Missouri Kansas City
Kansas City, Missouri, United States
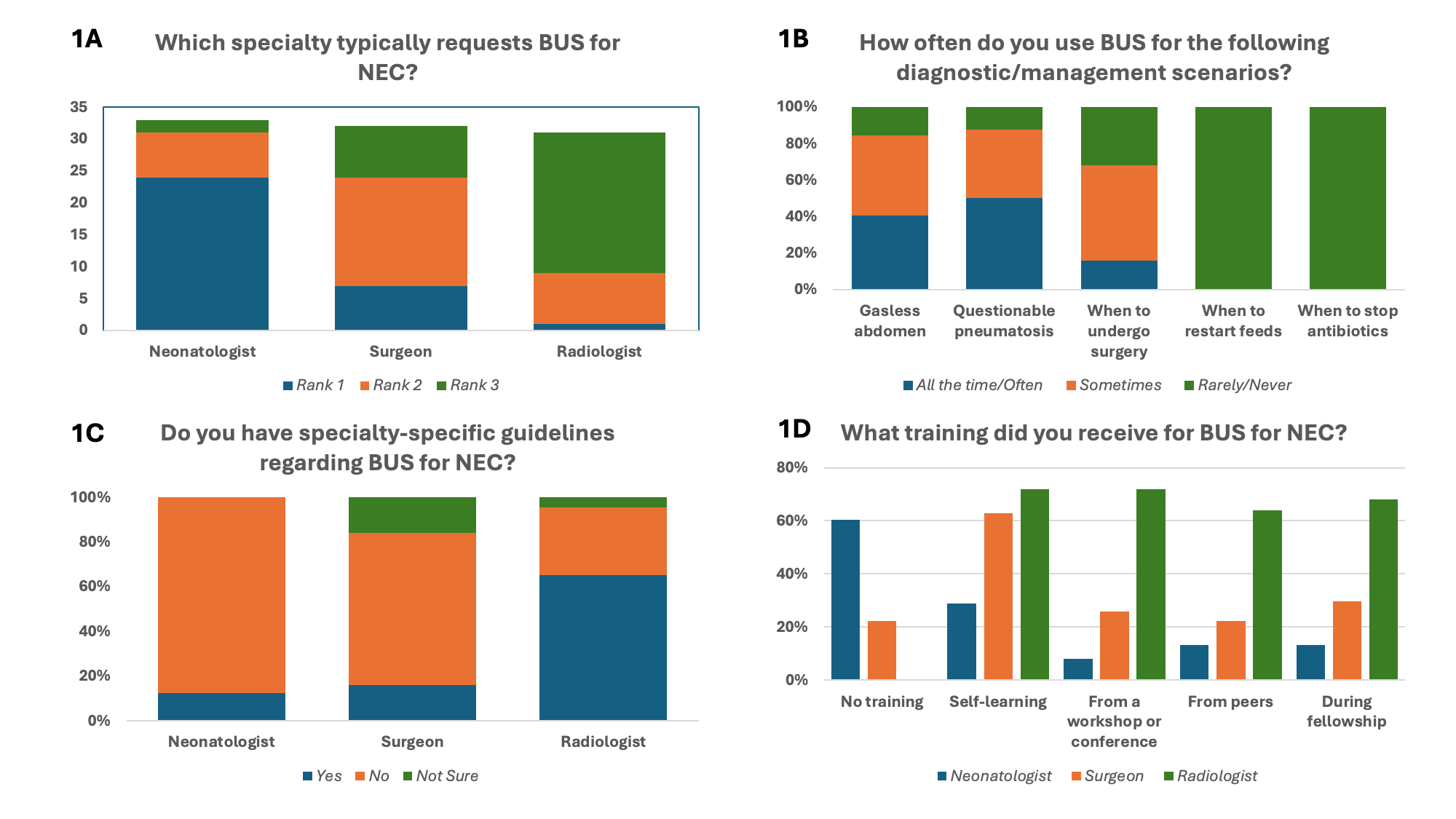 A: Users of BUS for NEC. Each responder was asked to rank which specialty typically requests BUS for NEC evaluations, with 1 being the most common and 3 being the least common B. Case-scenarios when BUS is used. C. Guidelines for using BUS across specialties. D. Training received regarding the use of BUS.
A: Users of BUS for NEC. Each responder was asked to rank which specialty typically requests BUS for NEC evaluations, with 1 being the most common and 3 being the least common B. Case-scenarios when BUS is used. C. Guidelines for using BUS across specialties. D. Training received regarding the use of BUS.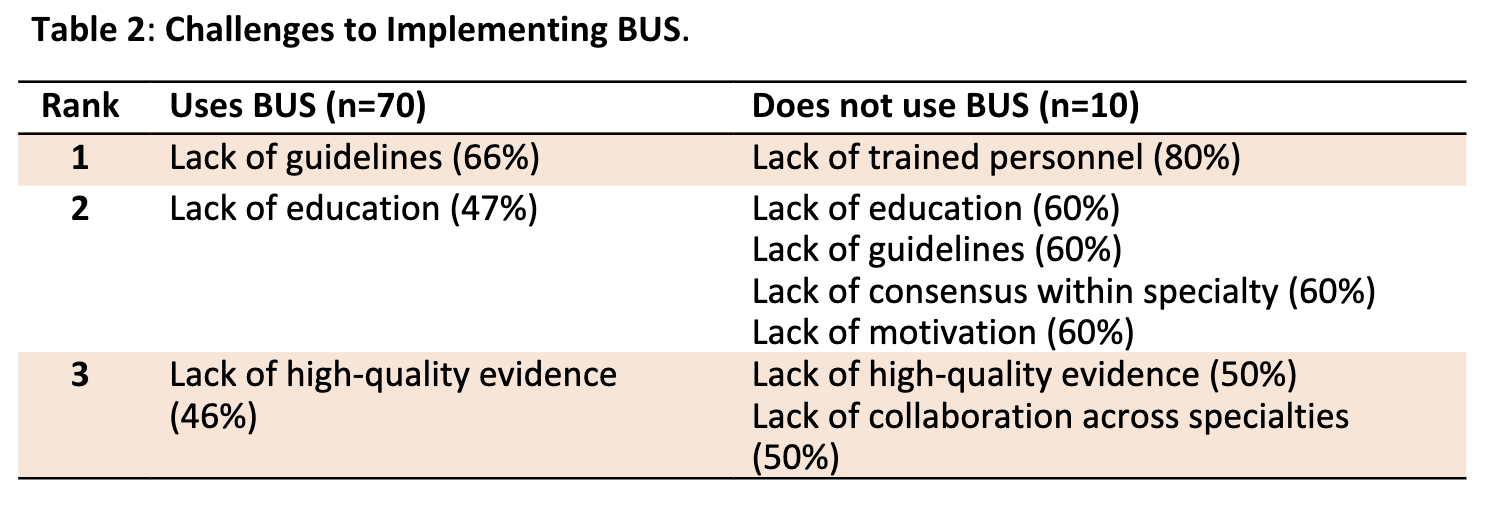 Top 3 perceived barriers to BUS among responders that use and do not use BUS at their site.
Top 3 perceived barriers to BUS among responders that use and do not use BUS at their site.