
Neonatal Fetal Nutrition & Metabolism 2
Session: Neonatal Fetal Nutrition & Metabolism 2
Dimitrios Angelis, MD (he/him/his)
Neonatologist
University of Texas Southwestern Medical School
Dallas, Texas, United States
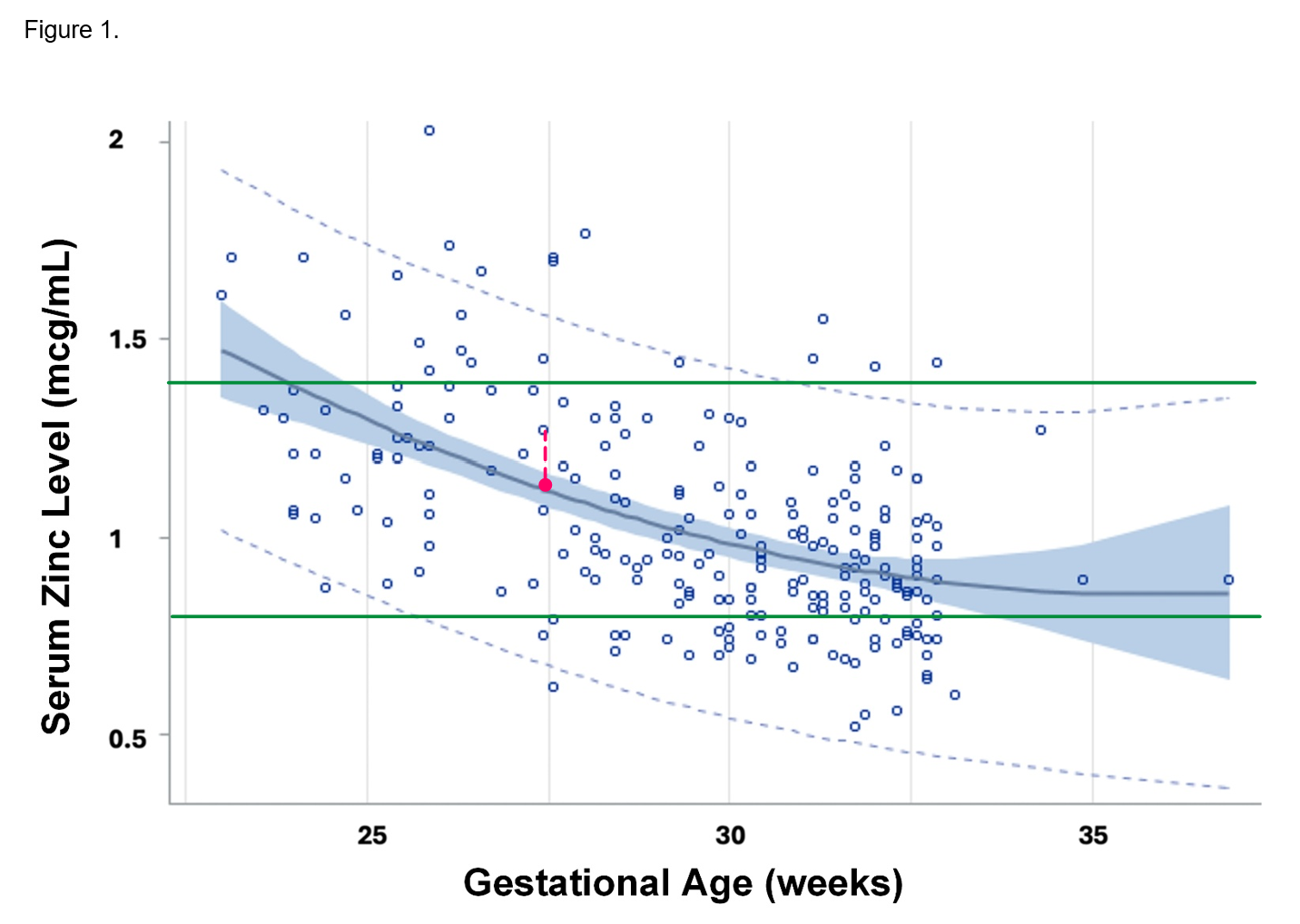 95% confidence and prediction intervals of first zinc level during the first 48 hours of life versus gestational age among infants <33 weeks gestational age or <1500 g birth weight, excluding those without congenital anomalies or comfort care only. Quadratic regression analysis. Adjusted R2=0.2921, n=228, P<0.0001. Equation: Zn = 5.63727 -0.26622 X GA +0.00370 x GA2. Green lines: currently accepted normative Zn values (0.74-1.46 mcc/dl). Red dashed line connects a measured Zn value (M) with its corresponding predicted (P- red dot). The M/P Zn ratio was calculated for each premature infant. Abbreviations: Zn, serum zinc concentration; GA, gestational age (weeks)
95% confidence and prediction intervals of first zinc level during the first 48 hours of life versus gestational age among infants <33 weeks gestational age or <1500 g birth weight, excluding those without congenital anomalies or comfort care only. Quadratic regression analysis. Adjusted R2=0.2921, n=228, P<0.0001. Equation: Zn = 5.63727 -0.26622 X GA +0.00370 x GA2. Green lines: currently accepted normative Zn values (0.74-1.46 mcc/dl). Red dashed line connects a measured Zn value (M) with its corresponding predicted (P- red dot). The M/P Zn ratio was calculated for each premature infant. Abbreviations: Zn, serum zinc concentration; GA, gestational age (weeks)
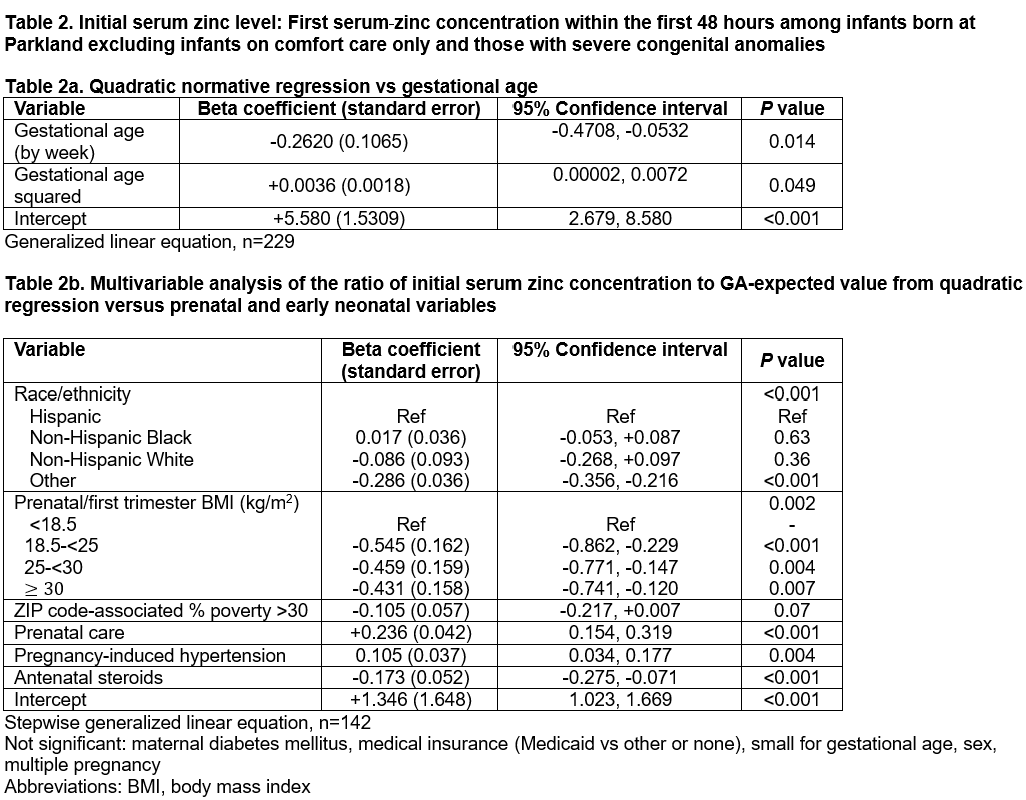 Stepwise generalized linear equation, n=142
Stepwise generalized linear equation, n=142