
Breastfeeding/Human Milk 1
Session: Breastfeeding/Human Milk 1
Kathryn Devadoss
Medical Student
University of Washington School of Medicine
Seattle, Washington, United States
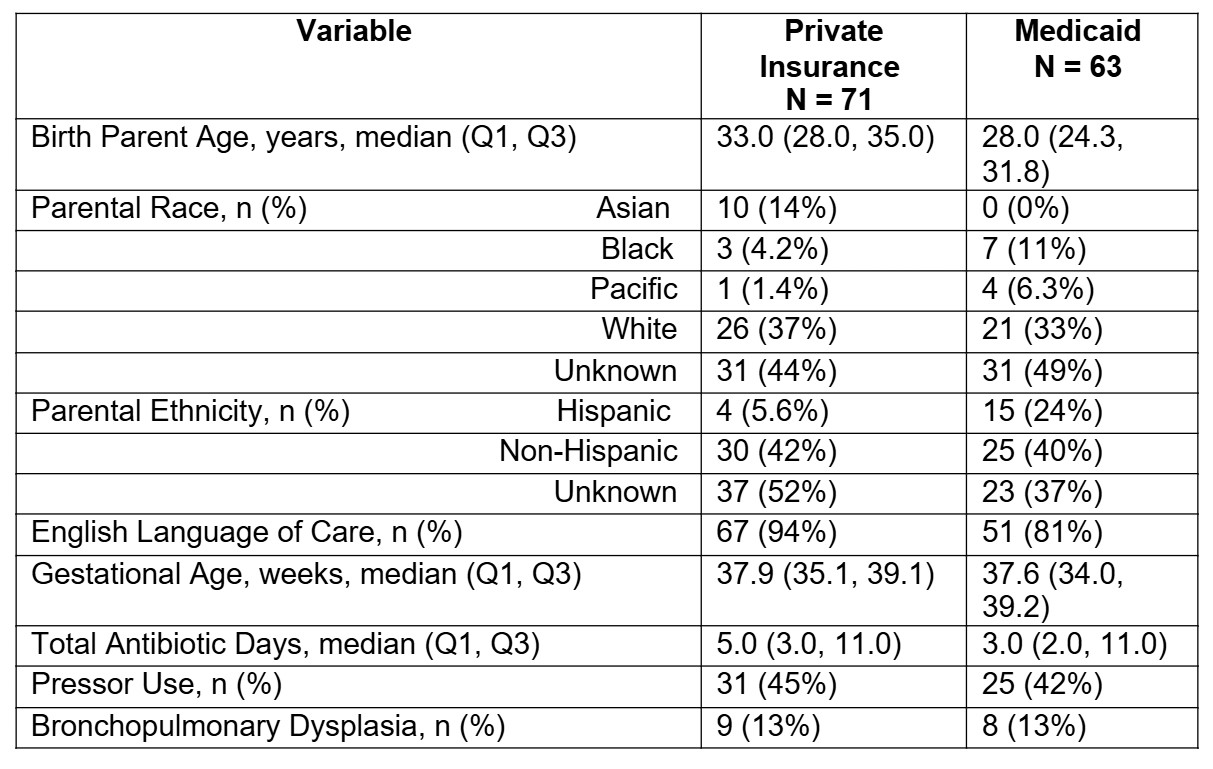 Cohort characteristics by parent insurance status on admission. Continuous variables are represented by median (IQR) and categorical variables by n (%). Bronchopulmonary dysplasia (BPD) was defined as a chronic lung disease that affects newborns, particularly those who are premature and require oxygen.
Cohort characteristics by parent insurance status on admission. Continuous variables are represented by median (IQR) and categorical variables by n (%). Bronchopulmonary dysplasia (BPD) was defined as a chronic lung disease that affects newborns, particularly those who are premature and require oxygen.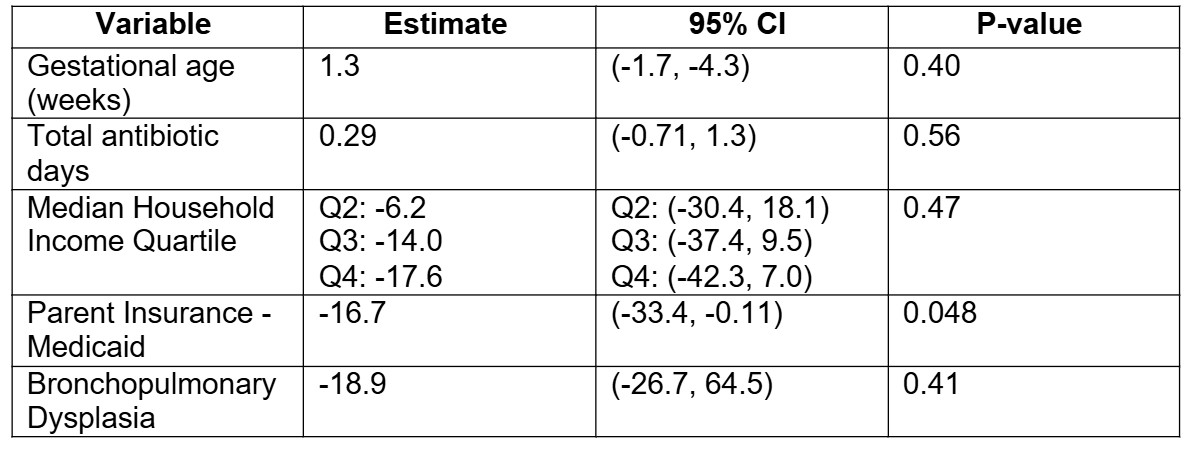 Multivariable linear regression model of total percentage of parent’s own milk during NICU hospitalization. Bronchopulmonary dysplasia (BPD) was defined as a chronic lung disease that affects newborns, particularly those who are premature and require oxygen. Median household income quartile was determined from zip code data obtained from the United States Census data.
Multivariable linear regression model of total percentage of parent’s own milk during NICU hospitalization. Bronchopulmonary dysplasia (BPD) was defined as a chronic lung disease that affects newborns, particularly those who are premature and require oxygen. Median household income quartile was determined from zip code data obtained from the United States Census data. 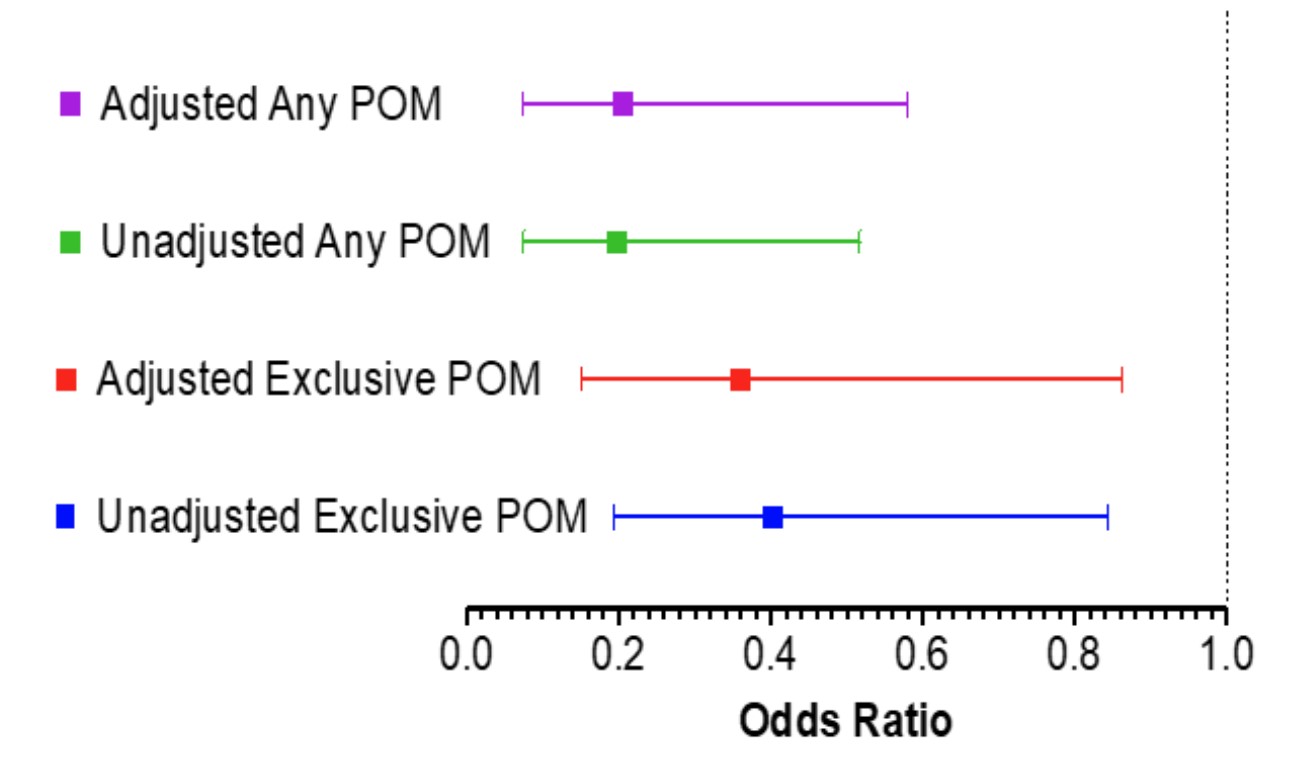 Forest plot of unadjusted and adjusted models of exclusive POM or any POM at NICU discharge. Models adjusted for gestational age, total antibiotic days, median household income, parent insurance status, and bronchopulmonary dysplasia.
Forest plot of unadjusted and adjusted models of exclusive POM or any POM at NICU discharge. Models adjusted for gestational age, total antibiotic days, median household income, parent insurance status, and bronchopulmonary dysplasia. 