
Infectious Diseases 3: Acute respiratory infections
Session: Infectious Diseases 3: Acute respiratory infections
Tyler Stephen, MD (he/him/his)
Fellow
University of Rochester School of Medicine and Dentistry
Rochester, New York, United States
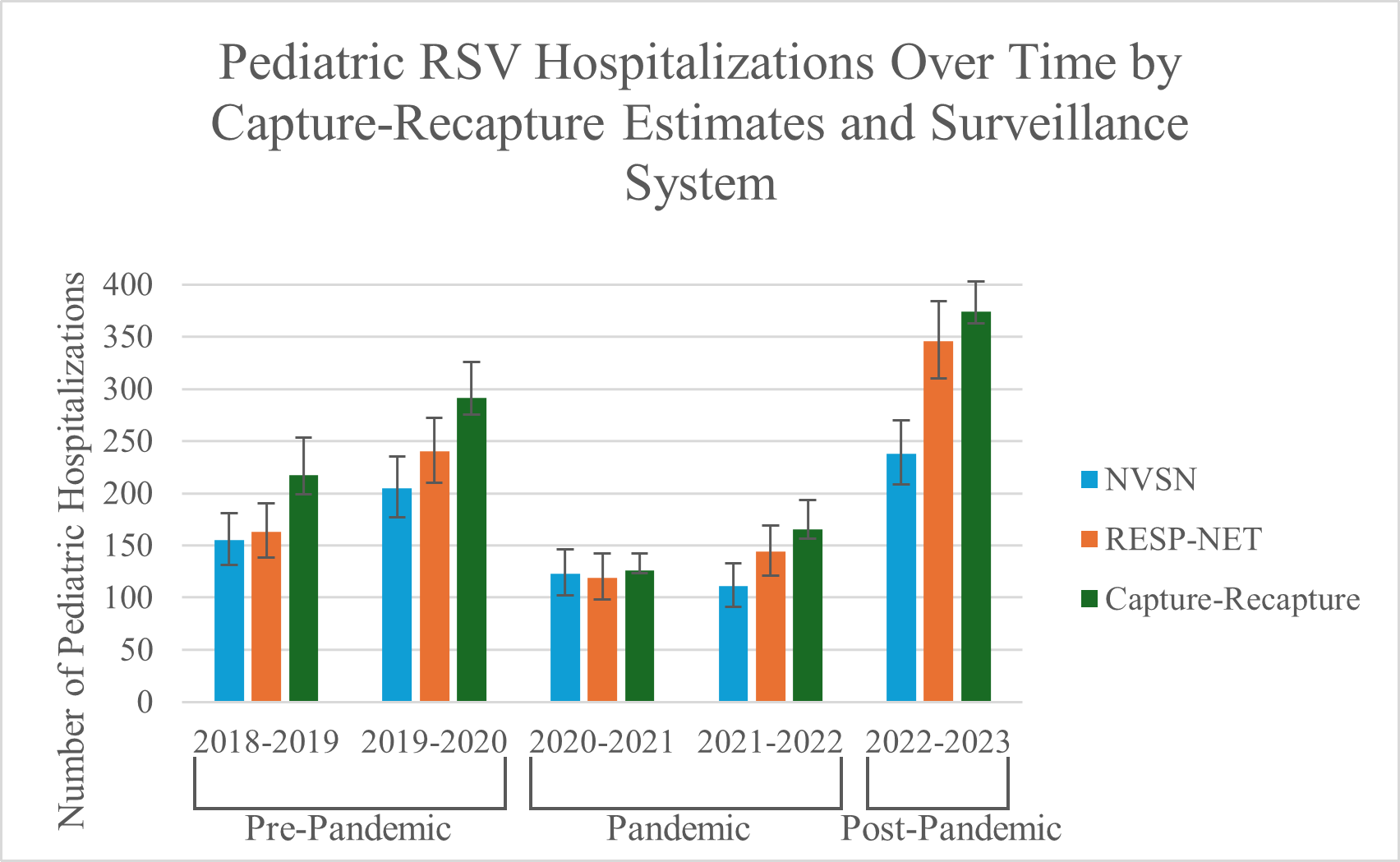 Pediatric RSV Hospitalizations Over Time by Capture-Recapture Estimates and Surveillance System
Pediatric RSV Hospitalizations Over Time by Capture-Recapture Estimates and Surveillance System  Estimated RSV Hospitalization Rates per 100,000 Children by Season and Age Based on Capture-Recapture Estimates
Estimated RSV Hospitalization Rates per 100,000 Children by Season and Age Based on Capture-Recapture Estimates Proportion of Estimated Capture-Recapture Hospitalizations Detected by Each Surveillance System
Proportion of Estimated Capture-Recapture Hospitalizations Detected by Each Surveillance System