
Hospital Medicine 5: Clinical
Session: Hospital Medicine 5: Clinical

Naseem Alammar, MD
Pediatric Hospital Medicine Fellow
University of Texas Southwestern & Children's Health
Dallas, Texas, United States
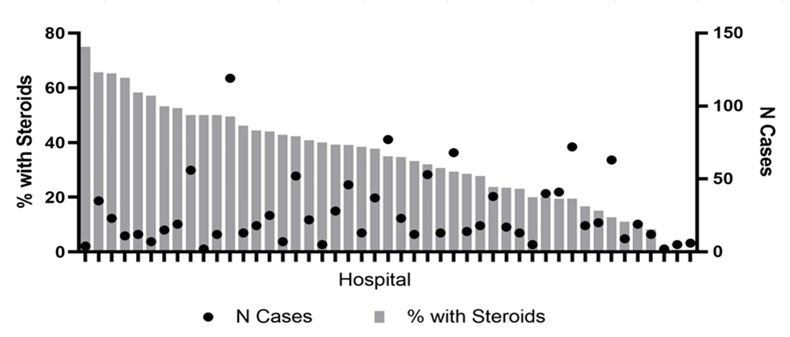 Figure 1. Rates of Systemic Steroid Use By Hospital
Figure 1. Rates of Systemic Steroid Use By Hospital.png) Table 1. Sociodemographic and Clinical Characteristics by Systemic Steroid Use
Table 1. Sociodemographic and Clinical Characteristics by Systemic Steroid Use 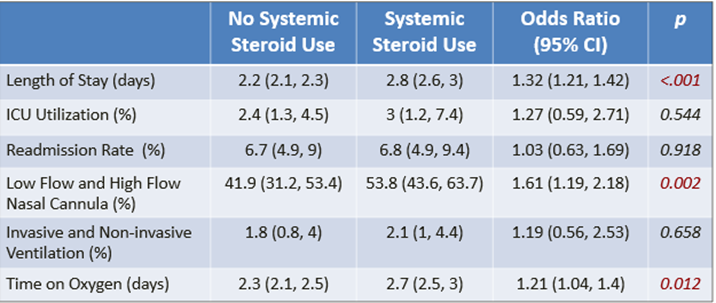 Table 2. Adjusted Outcomes by Systemic Steroid UseFigure 1. Rates of Systemic Steroid Use By HospitalTable 1. Sociodemographic and Clinical Characteristics by Systemic Steroid Use Table 2. Adjusted Outcomes by Systemic Steroid Use
Table 2. Adjusted Outcomes by Systemic Steroid UseFigure 1. Rates of Systemic Steroid Use By HospitalTable 1. Sociodemographic and Clinical Characteristics by Systemic Steroid Use Table 2. Adjusted Outcomes by Systemic Steroid Use