
Emergency Medicine 7
Session: Emergency Medicine 7
 photo")
Alexander M. Stephan, MD (he/him/his)
Assistant Professor of Clinical Emergency Medicine / Assistant Professor of Clinical Pediatrics
Weill Cornell Medicine
Brooklyn, New York, United States
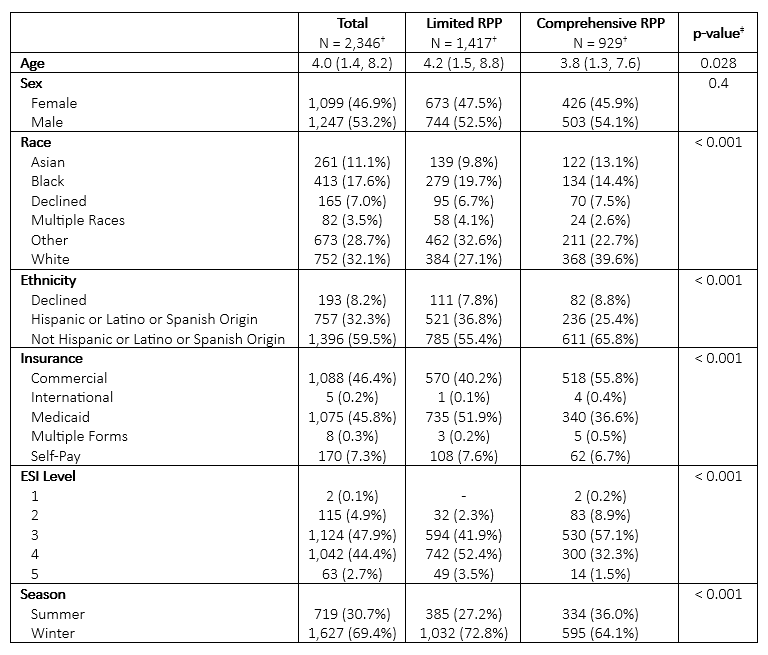 †Median (IQR); n (%)
†Median (IQR); n (%)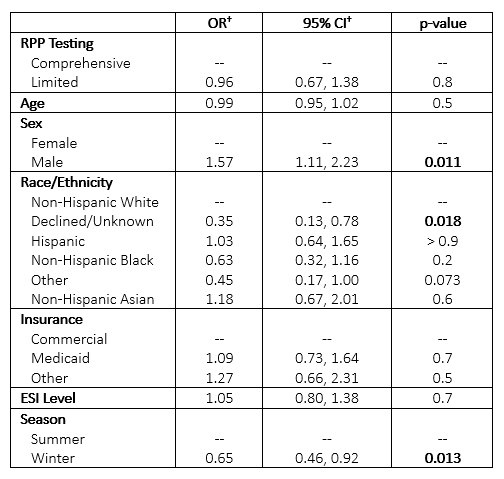 †OR = Odds Ratio, CI = Confidence Interval
†OR = Odds Ratio, CI = Confidence Interval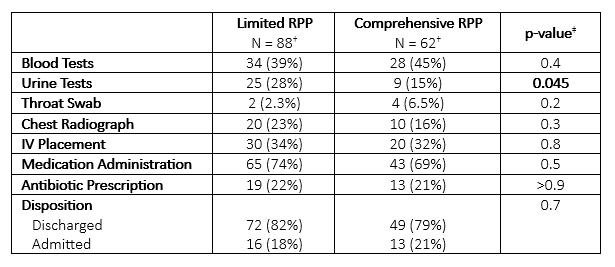 †n (%)†Median (IQR); n (%)†OR = Odds Ratio, CI = Confidence Interval†n (%)
†n (%)†Median (IQR); n (%)†OR = Odds Ratio, CI = Confidence Interval†n (%)