
Emergency Medicine 8
Session: Emergency Medicine 8

Katherine R. Genet, MD
Pediatric Emergency Medicine Fellow
Akron Children's Hospital
Akron, Ohio, United States
.jpg) Total patient encounters with type of febrile seizure, neurologic exam, and the subsequent neuroimaging (if obtained).
Total patient encounters with type of febrile seizure, neurologic exam, and the subsequent neuroimaging (if obtained).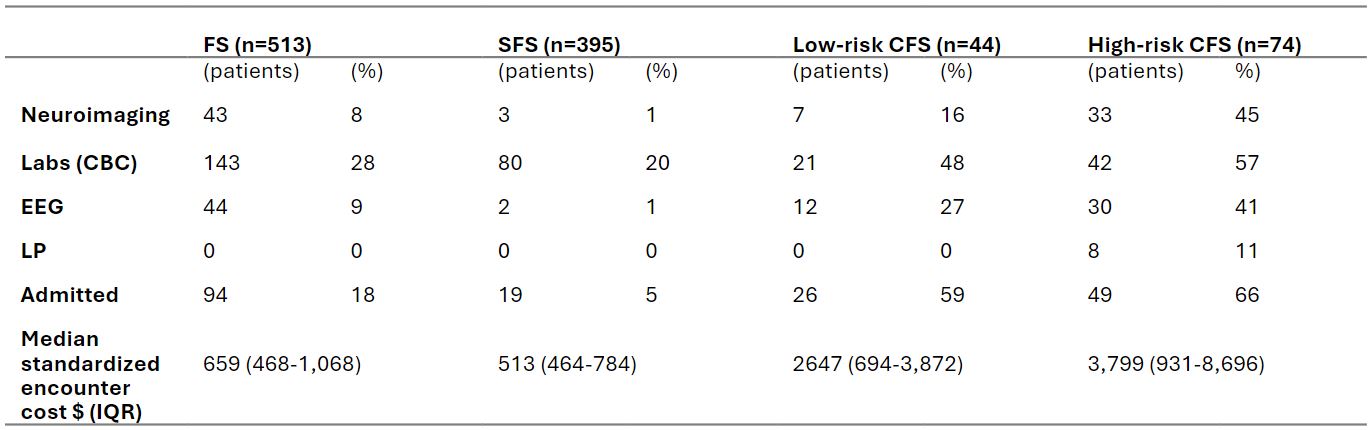 Number of patients to have neuroimaging, labs (CBC), EEGs, LP, admitted to the hospital, and median encounter cost of total FS, SFS, low-risk CFS, and high-risk CFS.
Number of patients to have neuroimaging, labs (CBC), EEGs, LP, admitted to the hospital, and median encounter cost of total FS, SFS, low-risk CFS, and high-risk CFS.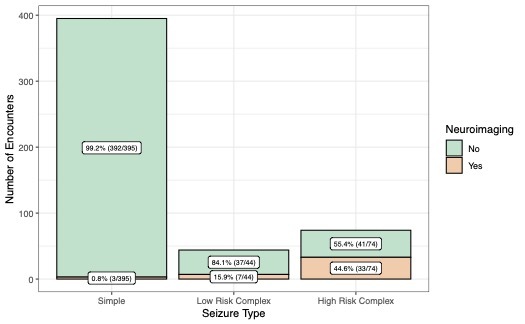 Number of encounters representing patients who had neuroimaging obtained classified by type of febrile seizure.
Number of encounters representing patients who had neuroimaging obtained classified by type of febrile seizure. 