
Endocrinology 2
Session: Endocrinology 2
 photo")
Rachel L. Palting, DO (she/her/hers)
Pediatric Endocrinology Fellow
Oregon Health & Science University
Portland, Oregon, United States
.png) Both patients presented with hypernatremia and hyperprolactinemia. Patient 1 was diagnosed with hypothyroidism based on decreased Free T4 from prior and cortisol deficiency based on ACTH stimulation test.
Both patients presented with hypernatremia and hyperprolactinemia. Patient 1 was diagnosed with hypothyroidism based on decreased Free T4 from prior and cortisol deficiency based on ACTH stimulation test. .png) Patient 1 had rapid increase in weight after diagnosis (16 kg over 5 months). Red arrow indicates initiation of dextroamphetamine-amphetamine. Rate of weight gain decreased after this intervention (6 kg over 13 months).
Patient 1 had rapid increase in weight after diagnosis (16 kg over 5 months). Red arrow indicates initiation of dextroamphetamine-amphetamine. Rate of weight gain decreased after this intervention (6 kg over 13 months).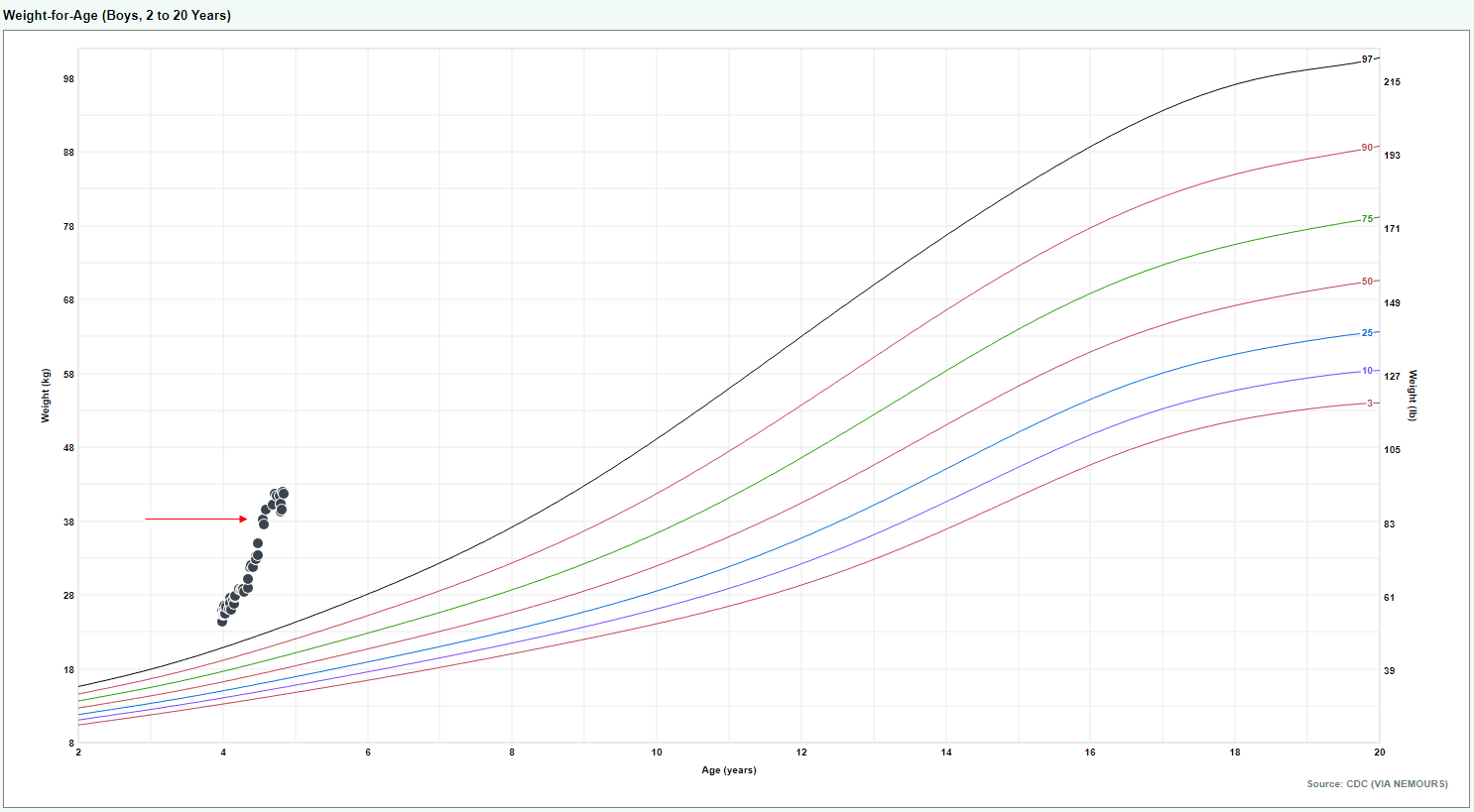 Patient 2 had rapid increase in weight after diagnosis (13.2 kg over 7 months). Red arrow indicates initiation of dextroamphetamine-amphetamine. Rate of weight gain decreased after this intervention (2 kg over 3 months).
Patient 2 had rapid increase in weight after diagnosis (13.2 kg over 7 months). Red arrow indicates initiation of dextroamphetamine-amphetamine. Rate of weight gain decreased after this intervention (2 kg over 3 months).