
Emergency Medicine 9
Session: Emergency Medicine 9
 photo")
Alexandra Licona-Freudenstein, MD (she/her/hers)
Fellow
University of Washington/ Seattle Children's Hospital
Seattle, Washington, United States
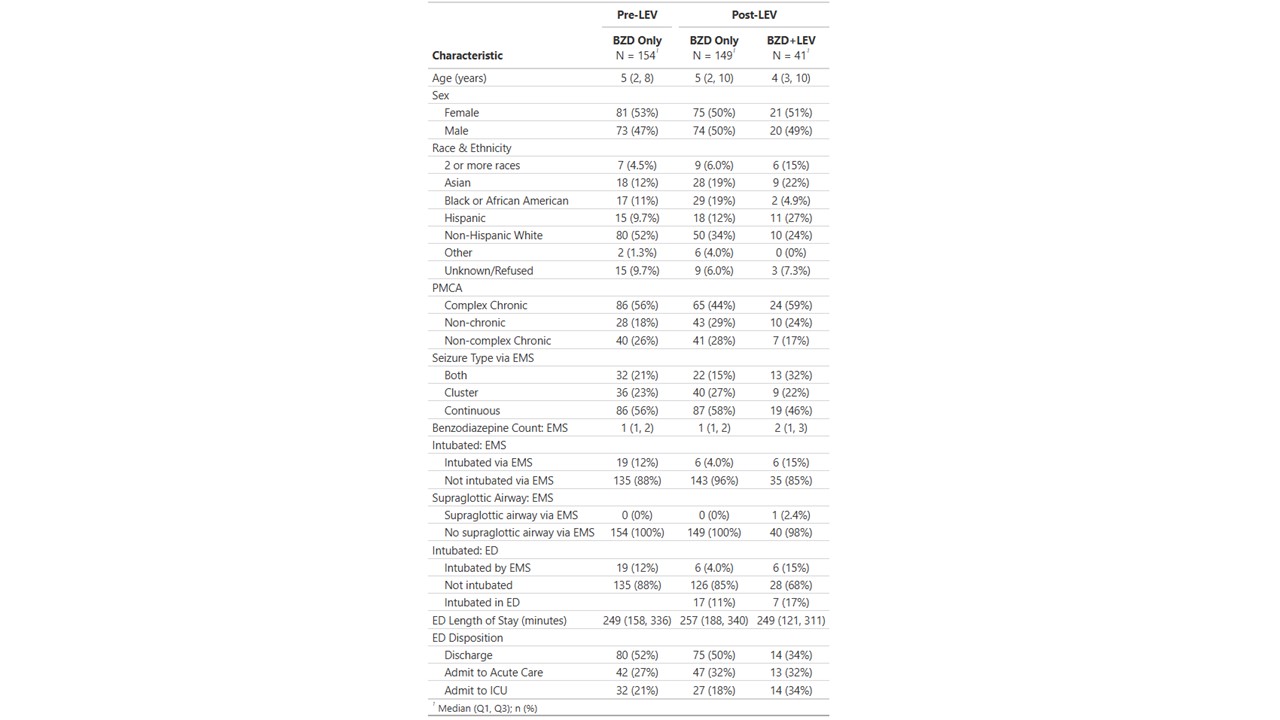 Patients are divided into 3 categories. Pre-LEV: received benzodiazepines only during baseline timeframe; post-LEV BZD only: received benzodiazepines only during intervention phase; post-LEV BZD+LEV: received benzodiazepine and levetiracetam during intervention phase
Patients are divided into 3 categories. Pre-LEV: received benzodiazepines only during baseline timeframe; post-LEV BZD only: received benzodiazepines only during intervention phase; post-LEV BZD+LEV: received benzodiazepine and levetiracetam during intervention phase