
Sedation Medicine
Session: Sedation Medicine
 photo")
Franklin Ducatez, MD, PHD (he/him/his)
Post-Doc
Boston Children's Hospital
Boston, Massachusetts, United States
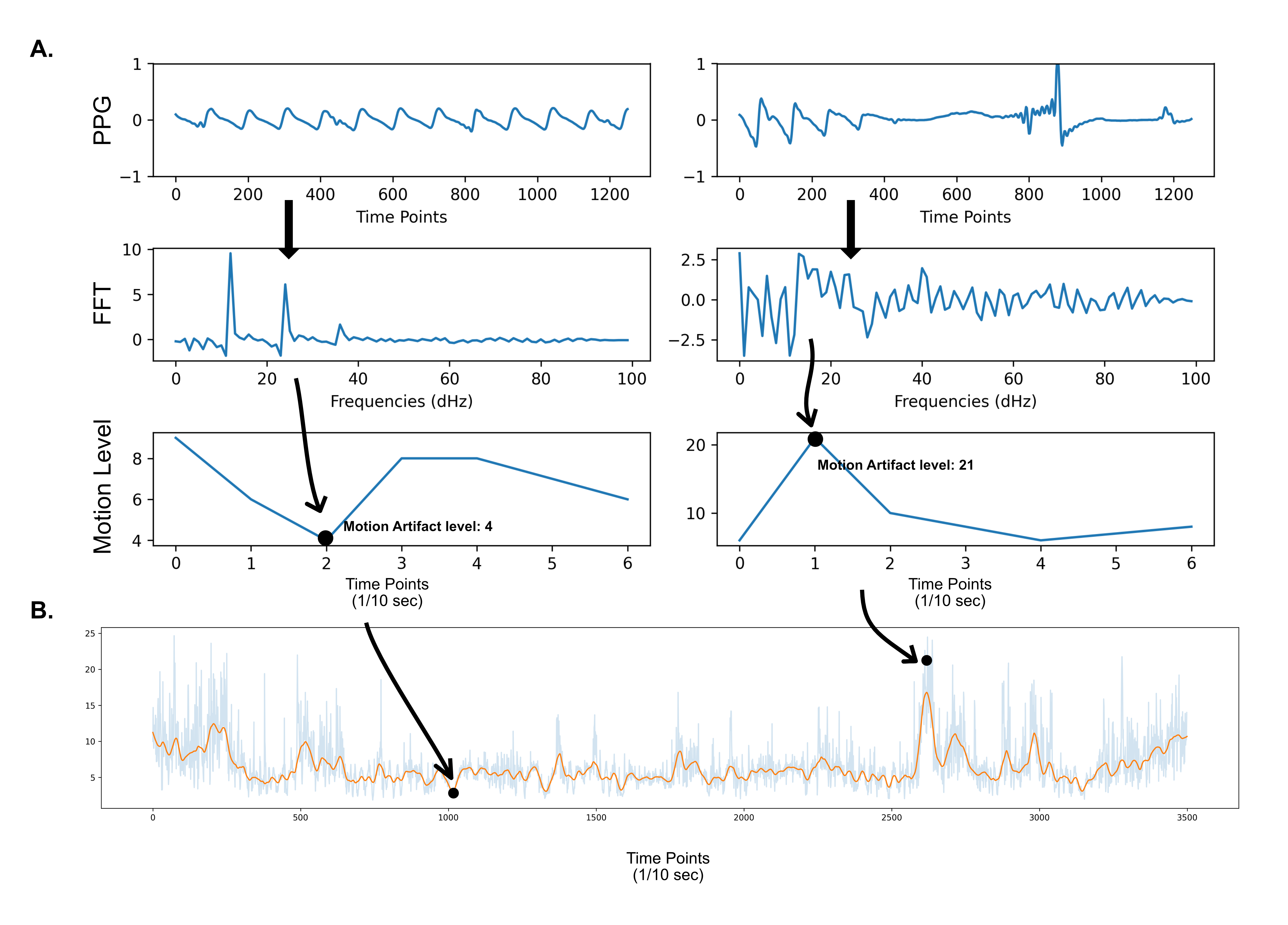 (A) Raw data from PPG are divided in 10 sec increments, then discrete Fourier transformation was performed. After normalisation and filtering, motion artifact level can be computed. (B) Evolution of this new metric accross a longer timespan (here 10h).
(A) Raw data from PPG are divided in 10 sec increments, then discrete Fourier transformation was performed. After normalisation and filtering, motion artifact level can be computed. (B) Evolution of this new metric accross a longer timespan (here 10h).