
Endocrinology 1
Session: Endocrinology 1
 photo")
Lauren E. Wisk, PhD (she/her/hers)
Assistant Professor
University of California, Los Angeles David Geffen School of Medicine
Los Angeles, California, United States
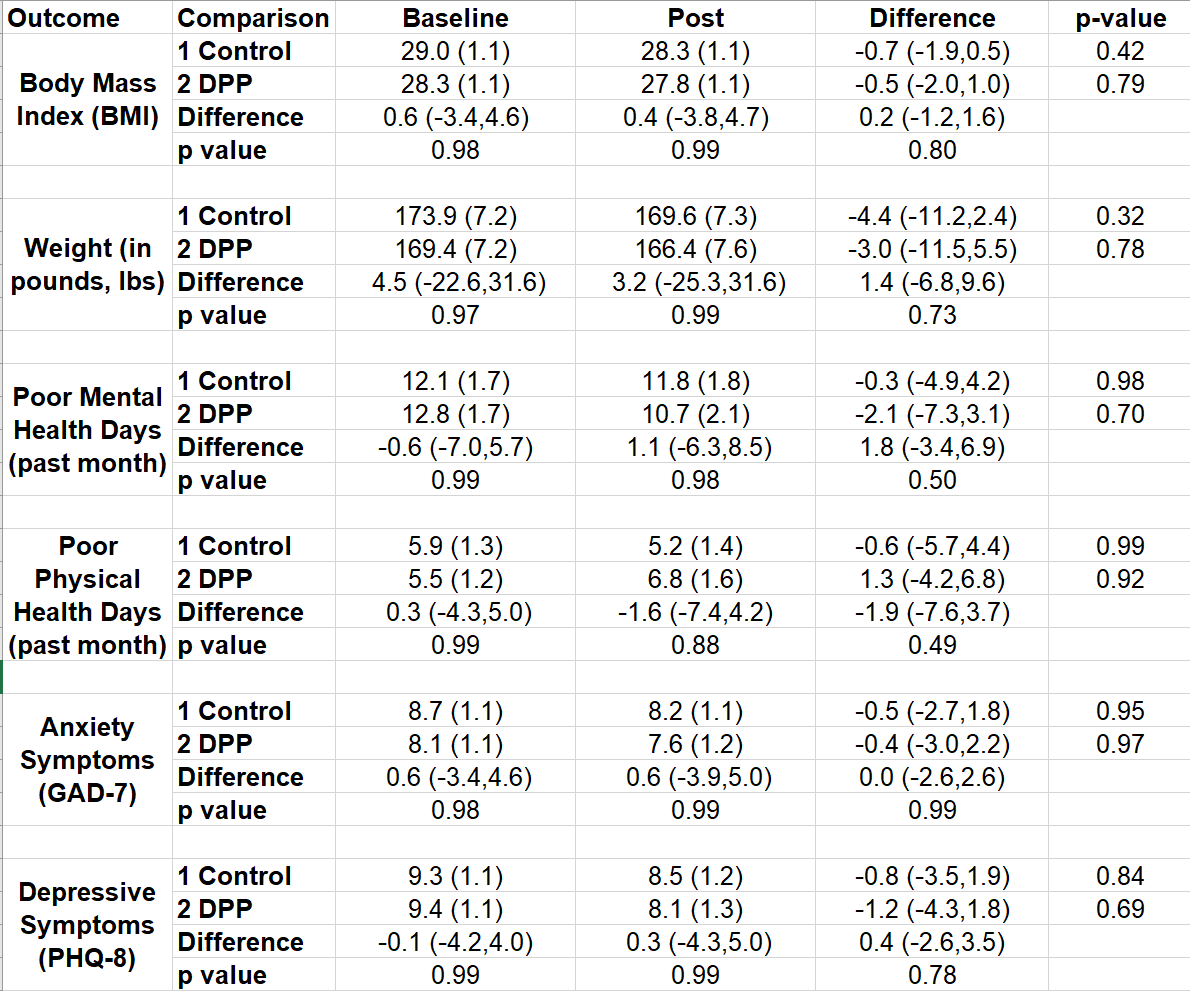 Table shows scores for each outcome (BMI, weight, poor mental health days, poor physical health days, GAD-7, PHQ-8) by group (treatment/DPP and control) and time (baseline and follow-up/post), as well as differences over time and within groups, derived from the mixed effects regression models. Models control for group, time, group by time interaction (the measure of the effect of the intervention relative to control), and repeated measures within individuals.
Table shows scores for each outcome (BMI, weight, poor mental health days, poor physical health days, GAD-7, PHQ-8) by group (treatment/DPP and control) and time (baseline and follow-up/post), as well as differences over time and within groups, derived from the mixed effects regression models. Models control for group, time, group by time interaction (the measure of the effect of the intervention relative to control), and repeated measures within individuals. 