
Palliative Care
Session: Palliative Care
 photo")
Aleksandra Olszewski, MD, MA (she/her/hers)
Faculty, Pediatric Critical Care
UPMC Childrens Hospital of Pittsburgh
Pittsburgh, Pennsylvania, United States
.jpg) Coding schematic with examples and exemplar quotes for each of the major codes.
Coding schematic with examples and exemplar quotes for each of the major codes.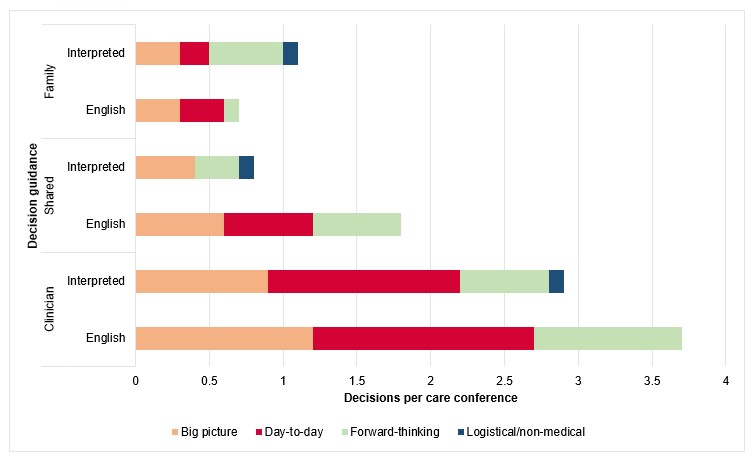 Number of decisions per care conference, by conference type (n= 18 (English); n=11 (interpreted)), decision type, and decision guidance.
Number of decisions per care conference, by conference type (n= 18 (English); n=11 (interpreted)), decision type, and decision guidance.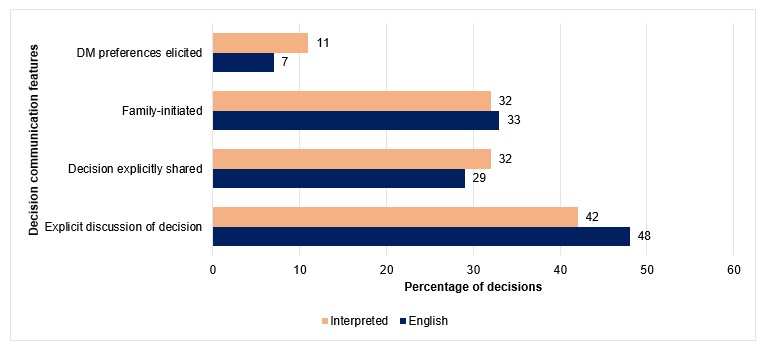 Percentage of decisions per care conference type (n=109 for English, n=53 for interpreted), by the following decision communication features: decision-making preferences elicited (p=0.4), decisions explicitly described (p=0.5), decisions explicitly described as shared (p=0.7), and decisions family-initiated (p=0.9).
Percentage of decisions per care conference type (n=109 for English, n=53 for interpreted), by the following decision communication features: decision-making preferences elicited (p=0.4), decisions explicitly described (p=0.5), decisions explicitly described as shared (p=0.7), and decisions family-initiated (p=0.9).