
Hospital Medicine 5: Clinical
Session: Hospital Medicine 5: Clinical
 photo")
Jared Kusma, MD, MS-CR (he/him/his)
Pediatric Hospitalist
Phoenix Children's
Phoenix Children's Hospital
Phoenix, Arizona, United States
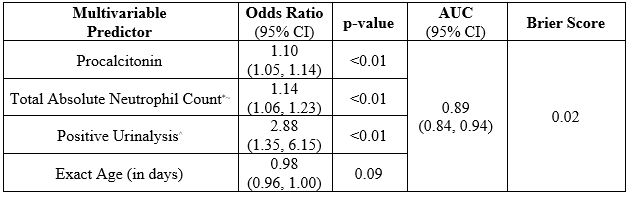 *: Total Absolute Neutrophil Count = Absolute Neutrophil Count + Band Count
*: Total Absolute Neutrophil Count = Absolute Neutrophil Count + Band Count  *: 3 patients missing a least 1 data point
*: 3 patients missing a least 1 data point 