
Emergency Medicine 8
Session: Emergency Medicine 8
 photo")
Rachel G. Hedstrom, MD (she/her/hers)
Pediatric Emergency Medicine Fellow
Children's Hospitals and Clinics of Minnesota
Saint Paul, Minnesota, United States
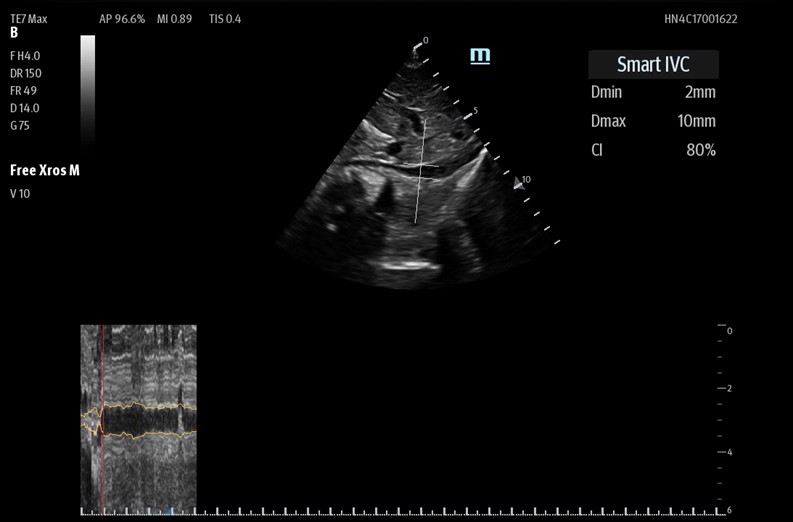 Utilizing the "Smart IVC" mode on the Mindray TE7 Max ultrasound machine.
Utilizing the "Smart IVC" mode on the Mindray TE7 Max ultrasound machine..jpg) Demographic and encounter-level characteristics.
Demographic and encounter-level characteristics.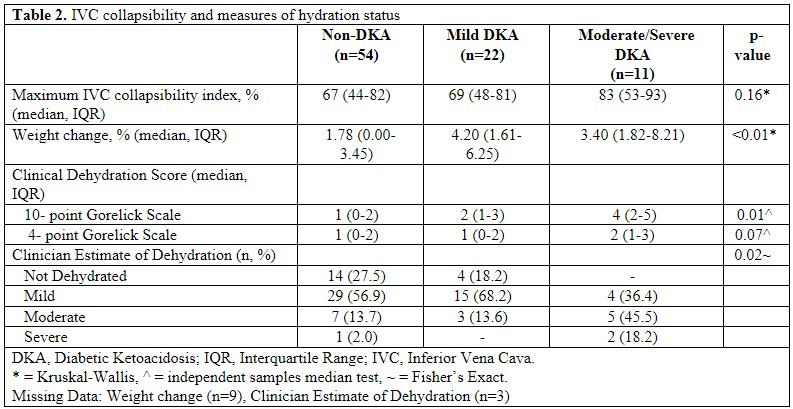 IVC Collapsibility and measures of hydration status.Utilizing the "Smart IVC" mode on the Mindray TE7 Max ultrasound machine.Demographic and encounter-level characteristics.IVC Collapsibility and measures of hydration status.
IVC Collapsibility and measures of hydration status.Utilizing the "Smart IVC" mode on the Mindray TE7 Max ultrasound machine.Demographic and encounter-level characteristics.IVC Collapsibility and measures of hydration status.