
Nephrology 5
Session: Nephrology 5
 photo")
Jared A. Martin (he/him/his)
Medical Student
Rocky Vista University School of Osteopathic Medicine
Tewksbury, Massachusetts, United States
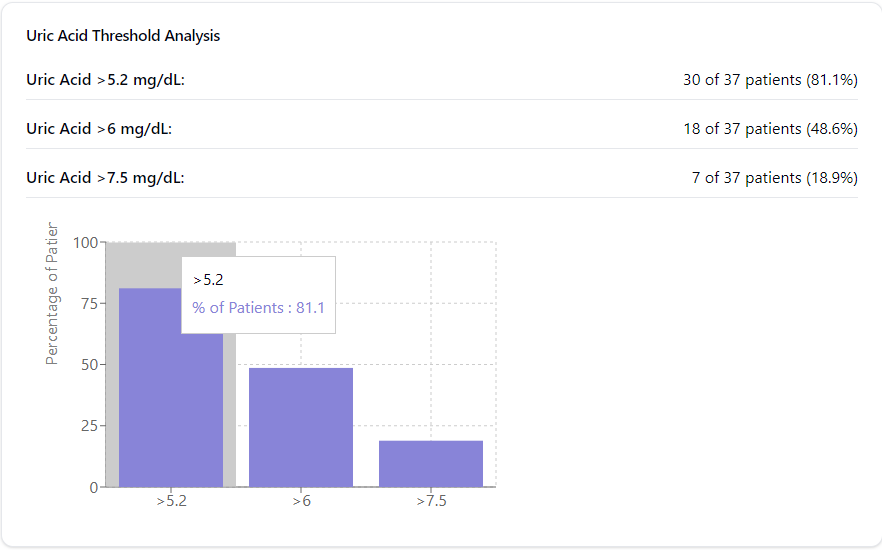 There is a slight positive correlation between uric acid and hematocrit. A significant portion of male patients (n = 37) have uric acid levels above a 5.2 mg/dL threshold.
There is a slight positive correlation between uric acid and hematocrit. A significant portion of male patients (n = 37) have uric acid levels above a 5.2 mg/dL threshold. The prevalence of elevated hematocrit (HCT ≥ 50) was 62.5% of all cases; the prevalence of obesity (BMI > 25) was 28.1% of all cases; the prevalence of elevated systolic blood pressure ≥ 130 was 15.6% of all cases. The strongest correlation was between hyperuricemia and elevated BMI (r = 0.42, p < 0.05).
The prevalence of elevated hematocrit (HCT ≥ 50) was 62.5% of all cases; the prevalence of obesity (BMI > 25) was 28.1% of all cases; the prevalence of elevated systolic blood pressure ≥ 130 was 15.6% of all cases. The strongest correlation was between hyperuricemia and elevated BMI (r = 0.42, p < 0.05).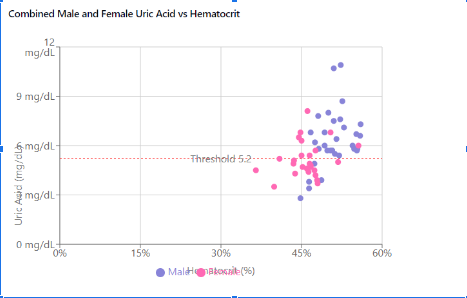 Data from adolescent patients at altitude (n = 80) demonstrate polycythemia and hyperuricemia, with 5.2 mg/dL as the threshold for hyperuricemia.
Data from adolescent patients at altitude (n = 80) demonstrate polycythemia and hyperuricemia, with 5.2 mg/dL as the threshold for hyperuricemia.