
Emergency Medicine 8
Session: Emergency Medicine 8

Andrea Rivera-Sepulveda, MD, MSc
Associate Professor
Nemours Children's Hospital
ORLANDO, Florida, United States
.png)
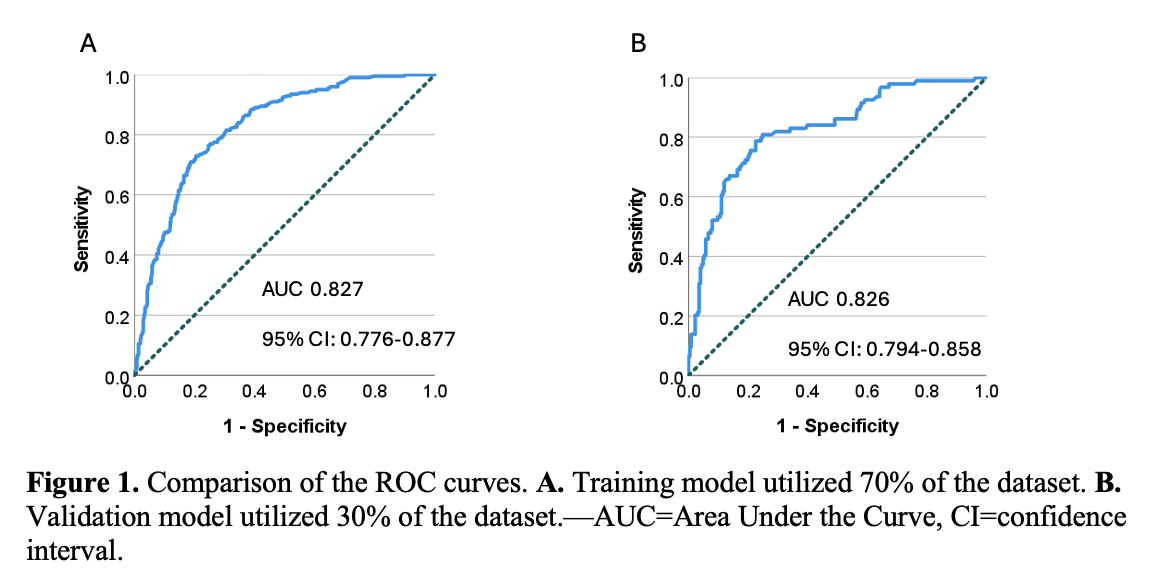 A. Training model utilized 70% of the dataset. B. Validation model utilized 30% of the dataset.—AUC=Area Under the Curve, CI=confidence interval.A. Training model utilized 70% of the dataset. B. Validation model utilized 30% of the dataset.—AUC=Area Under the Curve, CI=confidence interval.
A. Training model utilized 70% of the dataset. B. Validation model utilized 30% of the dataset.—AUC=Area Under the Curve, CI=confidence interval.A. Training model utilized 70% of the dataset. B. Validation model utilized 30% of the dataset.—AUC=Area Under the Curve, CI=confidence interval.