
Hospital Medicine 3: Systems/Population-based Research
Session: Hospital Medicine 3: Systems/Population-based Research
.jpg "Tammy Wang, BA (she/her/hers) photo")
Tammy Wang, BA (she/her/hers)
Medical Student
Hassenfeld Children's Hospital at NYU Langone, New York, United States
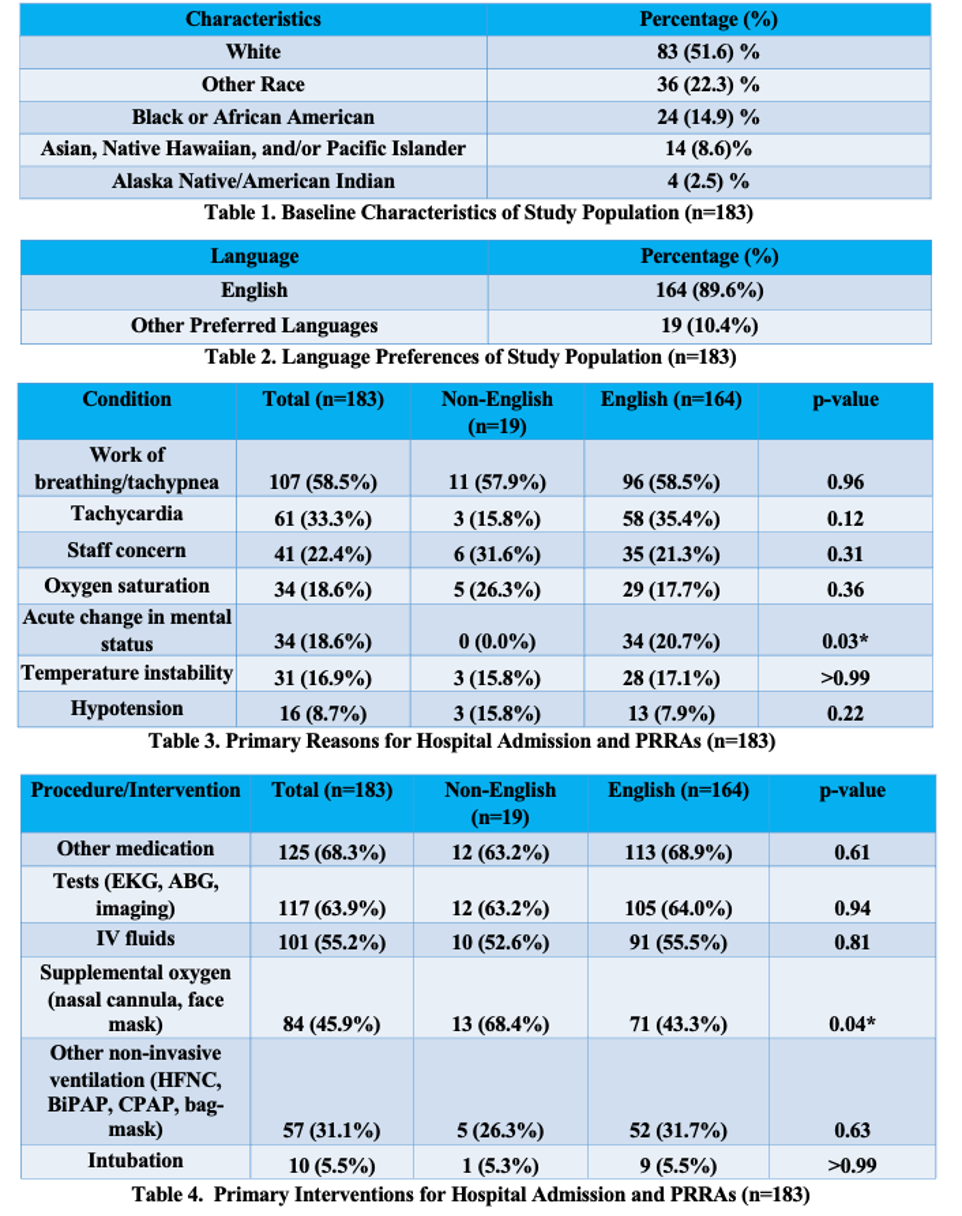 Table 1. Baseline Characteristics of Study Population
Table 1. Baseline Characteristics of Study Population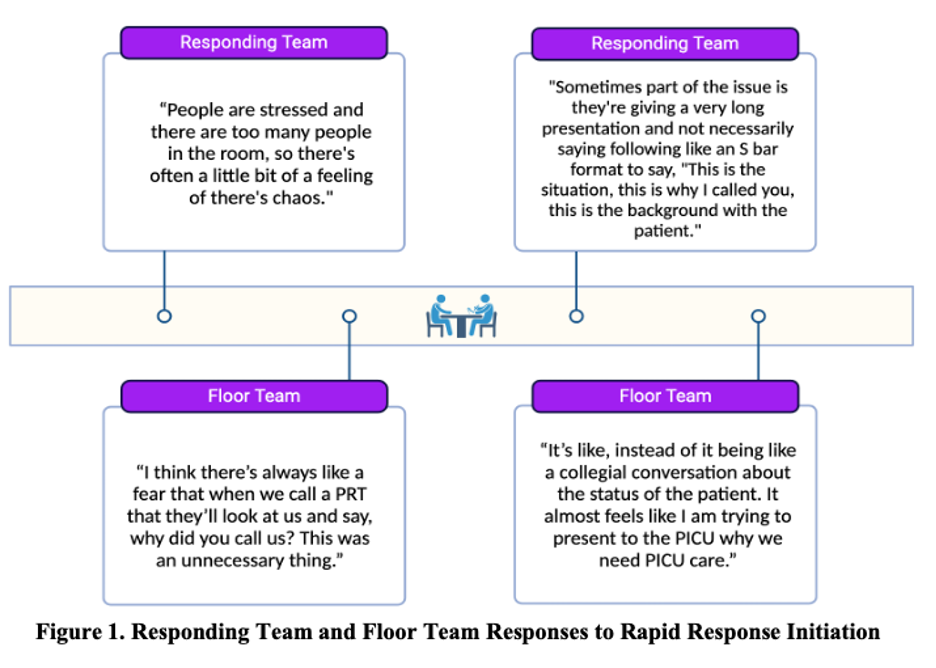 Responding Team and Floor Team Responses to Rapid Response Initiation
Responding Team and Floor Team Responses to Rapid Response Initiation