
Endocrinology 1
Session: Endocrinology 1
 photo")
Sheri VanOmen, MD (she/her/hers)
Clinical Assistant Professor, Neonatal-Perinatal Medicine
University of Michigan Medical School
Ann Arbor, Michigan, United States
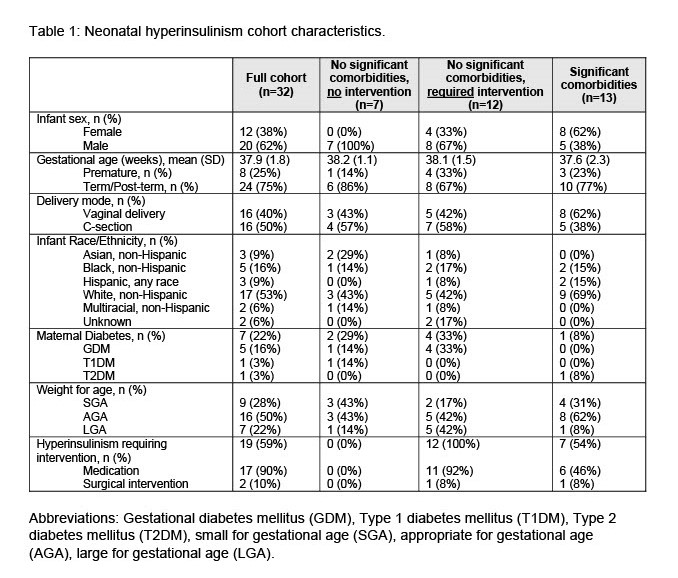 Abbreviations: Gestational diabetes mellitus (GDM), Type 1 diabetes mellitus (T1DM), Type 2 diabetes mellitus (T2DM), small for gestational age (SGA), appropriate for gestational age (AGA), large for gestational age (LGA).
Abbreviations: Gestational diabetes mellitus (GDM), Type 1 diabetes mellitus (T1DM), Type 2 diabetes mellitus (T2DM), small for gestational age (SGA), appropriate for gestational age (AGA), large for gestational age (LGA).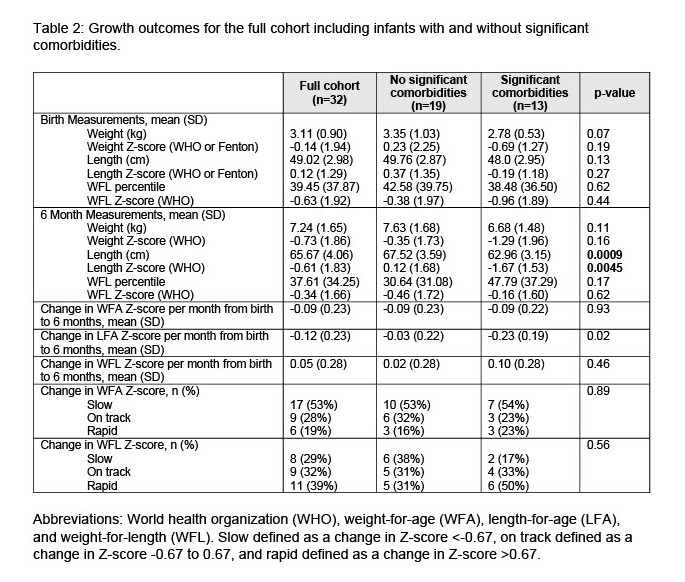 Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.
Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67..jpg) Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.Abbreviations: Gestational diabetes mellitus (GDM), Type 1 diabetes mellitus (T1DM), Type 2 diabetes mellitus (T2DM), small for gestational age (SGA), appropriate for gestational age (AGA), large for gestational age (LGA).Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.
Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.Abbreviations: Gestational diabetes mellitus (GDM), Type 1 diabetes mellitus (T1DM), Type 2 diabetes mellitus (T2DM), small for gestational age (SGA), appropriate for gestational age (AGA), large for gestational age (LGA).Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.Abbreviations: World health organization (WHO), weight-for-age (WFA), length-for-age (LFA), and weight-for-length (WFL). Slow defined as a change in Z-score <-0.67, on track defined as a change in Z-score -0.67 to 0.67, and rapid defined as a change in Z-score >0.67.