
Gastroenterology/Hepatology
Session: Gastroenterology/Hepatology
Aamer Imdad, MBBS, MPH (he/him/his)
University of Iowa Stead Family Children's Hospital
Iowa City, Iowa, United States
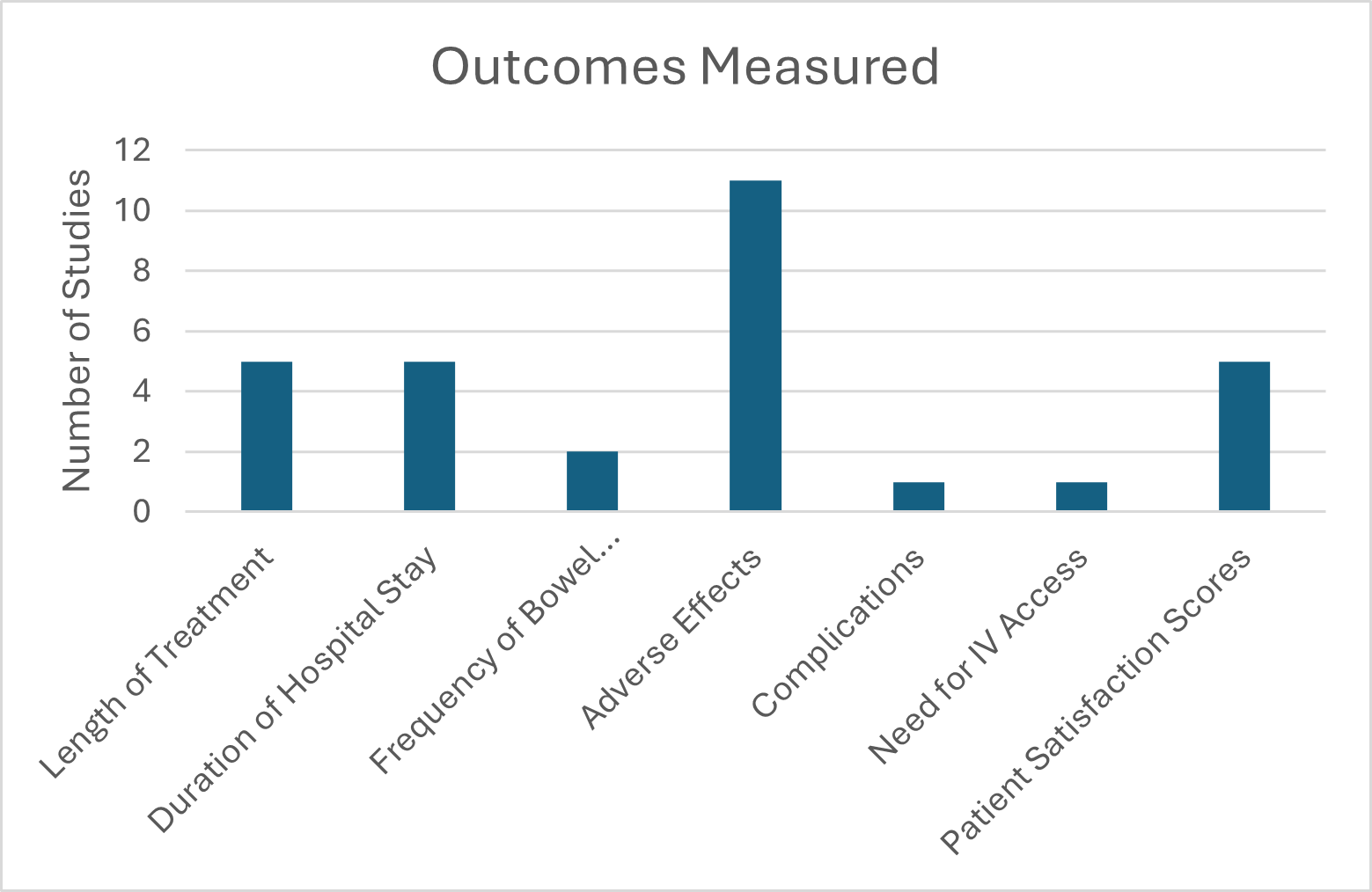 Outcomes measured during study.
Outcomes measured during study. 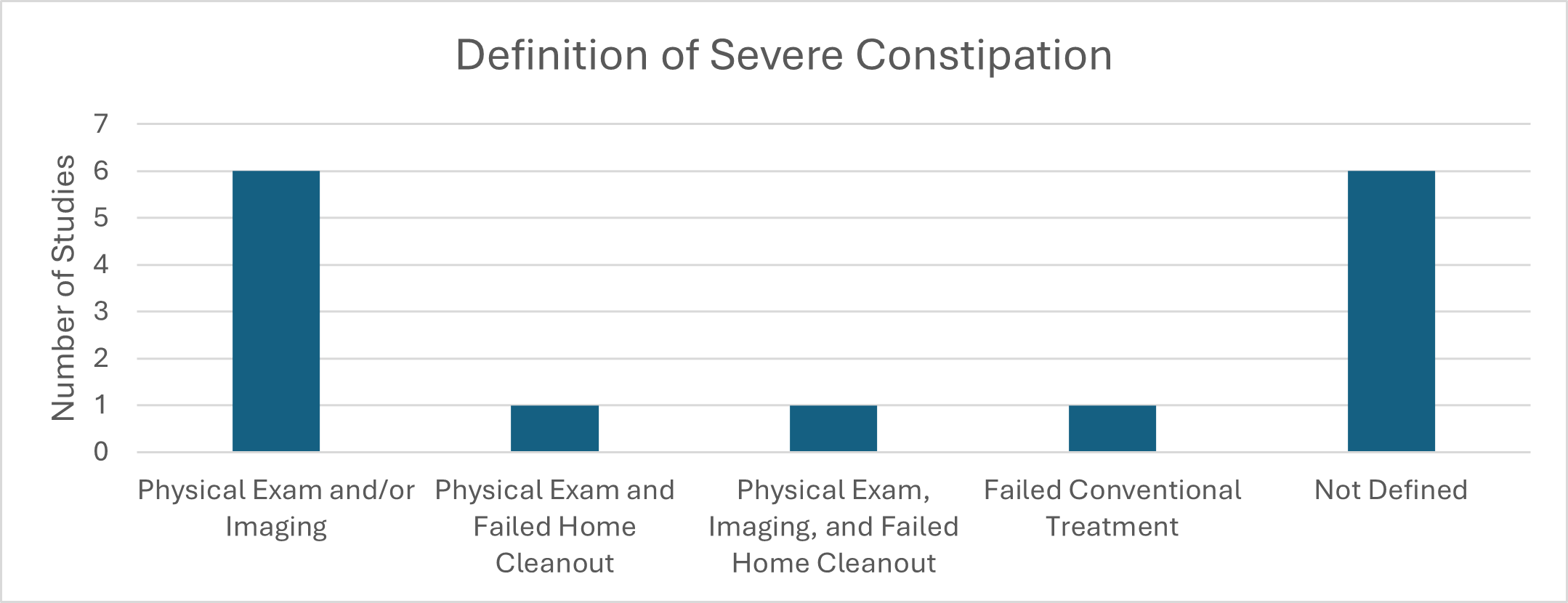 Definition of severe constipation based on included studies.
Definition of severe constipation based on included studies.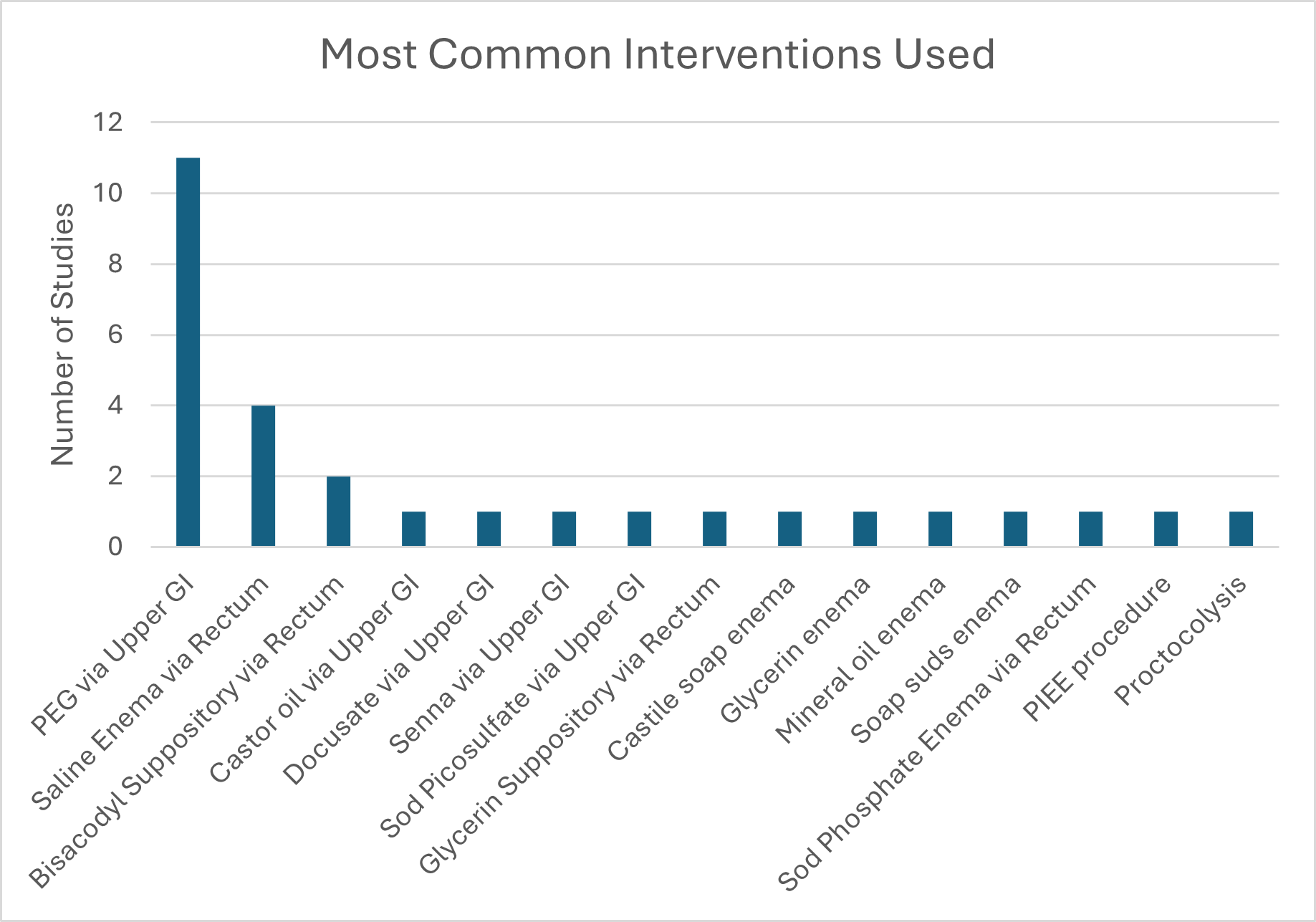 Most common interventions used in the studies for colon cleanout
Most common interventions used in the studies for colon cleanout