
Neonatal Neurology 5: Fetal
Session: Neonatal Neurology 5: Fetal
.jpg "John D. E Barks, MD (he/him/his) photo")
John D. E Barks, MD (he/him/his)
Professor
University of Michigan Medical School
Ann Arbor, Michigan, United States
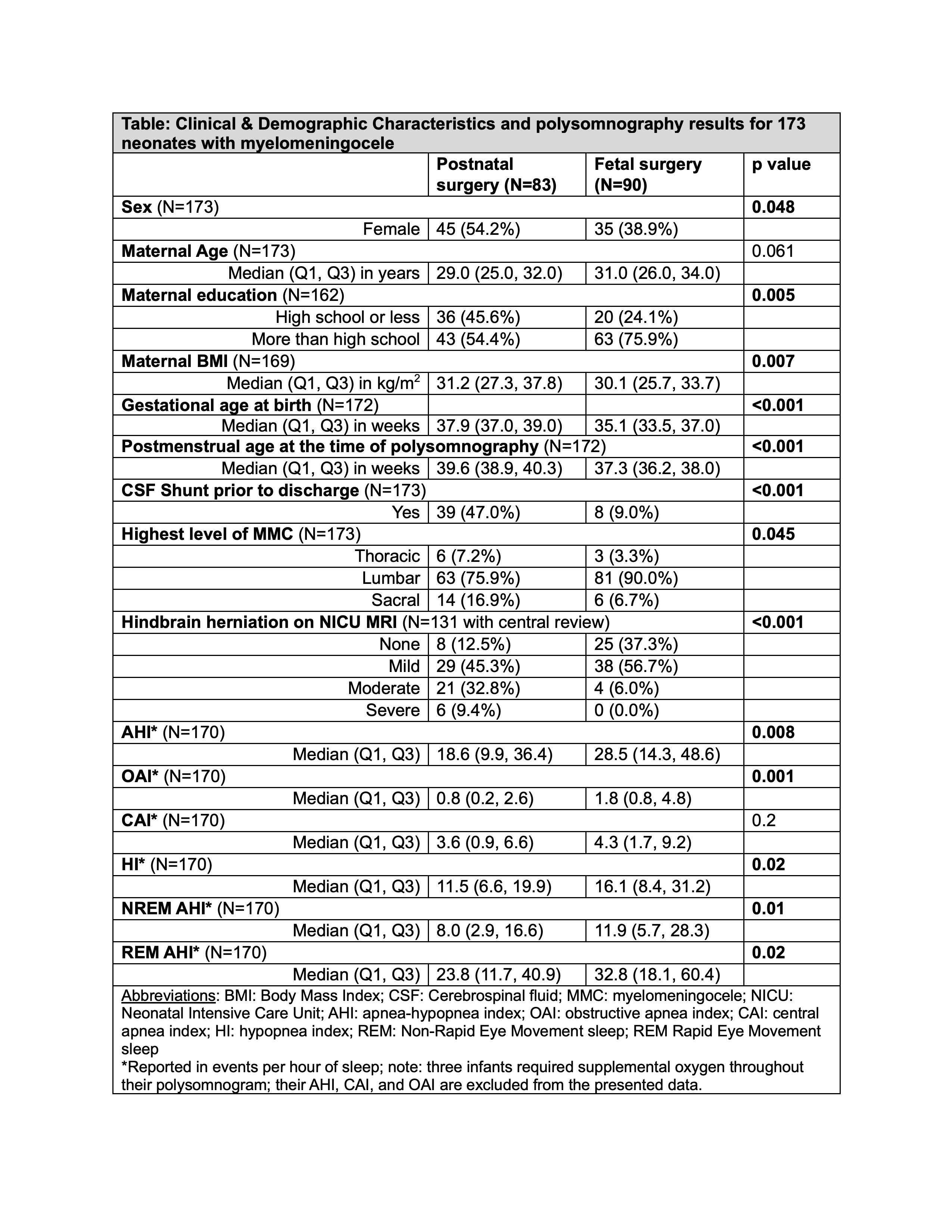 Clinical and demographic characteristics and polysomnography results for 173 neonates with myelomeningocele
Clinical and demographic characteristics and polysomnography results for 173 neonates with myelomeningocele Distribution of sleep disorders among 173 neonates with myelomeningocele (infants can have more than one diagnosis). Normal polysomnograms were recorded in 81/173 (47%).
Distribution of sleep disorders among 173 neonates with myelomeningocele (infants can have more than one diagnosis). Normal polysomnograms were recorded in 81/173 (47%). Distribution of Apnea-Hypopnea Index (AHI), Central Apnea Index (CAI), and Obstructive Apnea Index (OAI) among 173 neonates with myelomeningocele who underwent bedside polysomnography at >35 weeks post-menstrual age, prior to hospital discharge.Clinical and demographic characteristics and polysomnography results for 173 neonates with myelomeningoceleDistribution of sleep disorders among 173 neonates with myelomeningocele (infants can have more than one diagnosis). Normal polysomnograms were recorded in 81/173 (47%).Distribution of Apnea-Hypopnea Index (AHI), Central Apnea Index (CAI), and Obstructive Apnea Index (OAI) among 173 neonates with myelomeningocele who underwent bedside polysomnography at >35 weeks post-menstrual age, prior to hospital discharge.
Distribution of Apnea-Hypopnea Index (AHI), Central Apnea Index (CAI), and Obstructive Apnea Index (OAI) among 173 neonates with myelomeningocele who underwent bedside polysomnography at >35 weeks post-menstrual age, prior to hospital discharge.Clinical and demographic characteristics and polysomnography results for 173 neonates with myelomeningoceleDistribution of sleep disorders among 173 neonates with myelomeningocele (infants can have more than one diagnosis). Normal polysomnograms were recorded in 81/173 (47%).Distribution of Apnea-Hypopnea Index (AHI), Central Apnea Index (CAI), and Obstructive Apnea Index (OAI) among 173 neonates with myelomeningocele who underwent bedside polysomnography at >35 weeks post-menstrual age, prior to hospital discharge.