
Environmental Health 1
Session: Environmental Health 1
 photo")
Timothy Nelin, MD (he/him/his)
Attending Physician
Childrens Hospital of Philadelphia
Philadelphia, Pennsylvania, United States
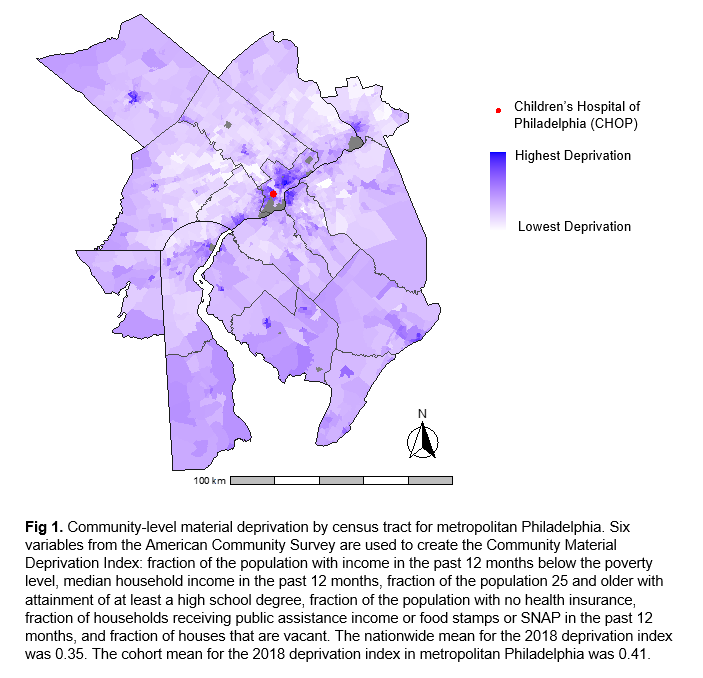 Community-level material deprivation by census tract for metropolitan Philadelphia. Six variables from the American Community Survey are used to create the Community Material Deprivation Index: fraction of the population with income in the past 12 months below the poverty level, median household income in the past 12 months, fraction of the population 25 and older with attainment of at least a high school degree, fraction of the population with no health insurance, fraction of households receiving public assistance income or food stamps or SNAP in the past 12 months, and fraction of houses that are vacant. The nationwide mean for the 2018 deprivation index was 0.35. The cohort mean for the 2018 deprivation index in metropolitan Philadelphia was 0.41.Community-level material deprivation by census tract for metropolitan Philadelphia. Six variables from the American Community Survey are used to create the Community Material Deprivation Index: fraction of the population with income in the past 12 months below the poverty level, median household income in the past 12 months, fraction of the population 25 and older with attainment of at least a high school degree, fraction of the population with no health insurance, fraction of households receiving public assistance income or food stamps or SNAP in the past 12 months, and fraction of houses that are vacant. The nationwide mean for the 2018 deprivation index was 0.35. The cohort mean for the 2018 deprivation index in metropolitan Philadelphia was 0.41.
Community-level material deprivation by census tract for metropolitan Philadelphia. Six variables from the American Community Survey are used to create the Community Material Deprivation Index: fraction of the population with income in the past 12 months below the poverty level, median household income in the past 12 months, fraction of the population 25 and older with attainment of at least a high school degree, fraction of the population with no health insurance, fraction of households receiving public assistance income or food stamps or SNAP in the past 12 months, and fraction of houses that are vacant. The nationwide mean for the 2018 deprivation index was 0.35. The cohort mean for the 2018 deprivation index in metropolitan Philadelphia was 0.41.Community-level material deprivation by census tract for metropolitan Philadelphia. Six variables from the American Community Survey are used to create the Community Material Deprivation Index: fraction of the population with income in the past 12 months below the poverty level, median household income in the past 12 months, fraction of the population 25 and older with attainment of at least a high school degree, fraction of the population with no health insurance, fraction of households receiving public assistance income or food stamps or SNAP in the past 12 months, and fraction of houses that are vacant. The nationwide mean for the 2018 deprivation index was 0.35. The cohort mean for the 2018 deprivation index in metropolitan Philadelphia was 0.41.