
Nephrology 6
Session: Nephrology 6
 photo")
Alexander J. Wolf, MD (he/him/his)
Fellow, Pediatric Nephrology
Lucile Packard Children's Hospital Stanford
San Francisco, California, United States
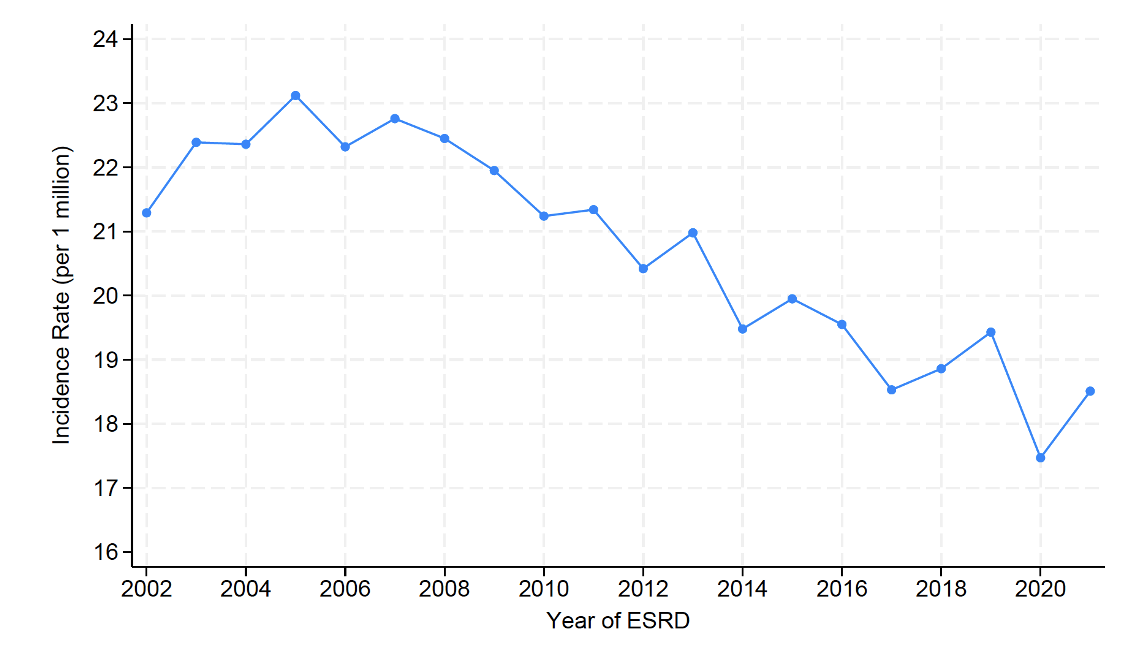 Incidence of ESRD from 2002-2021 in patients aged 0-24 by all causes.
Incidence of ESRD from 2002-2021 in patients aged 0-24 by all causes.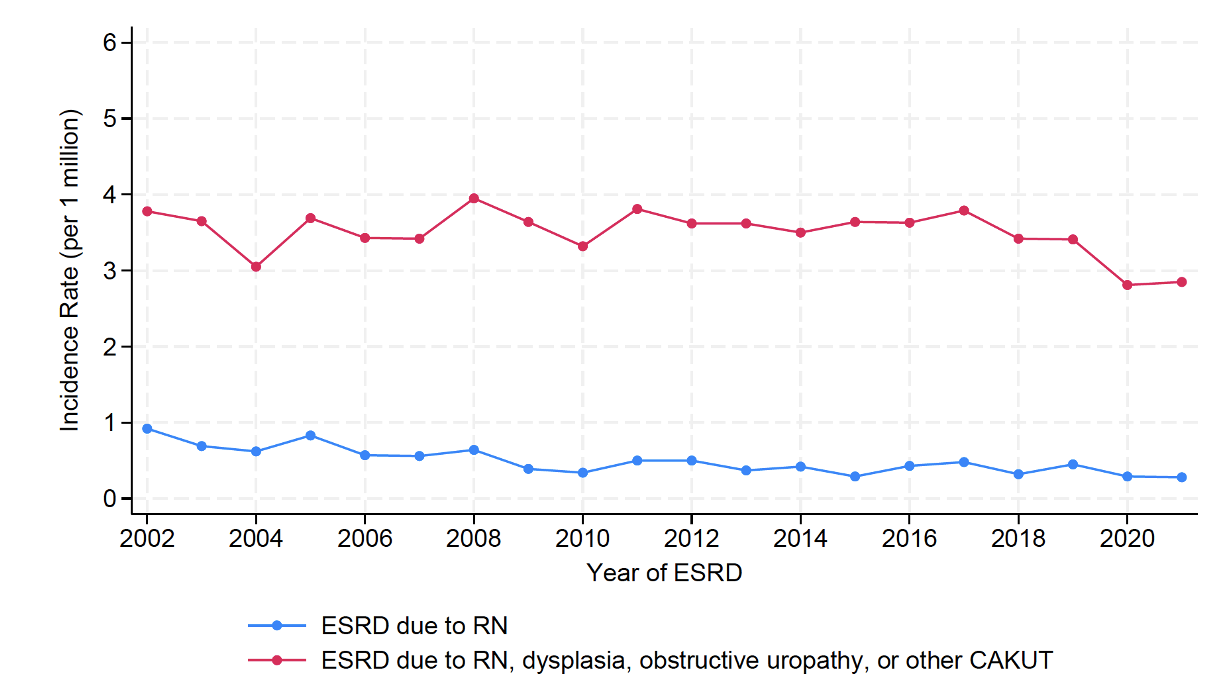 Incidence of ESRD from 2002-2021 in patients aged 0-24 due to reflux nephropathy and combined reflux nephropathy with overlapping diagnoses (dysplasia, obstructive uropathies, and other CAKUTs).Incidence of ESRD from 2002-2021 in patients aged 0-24 by all causes.Incidence of ESRD from 2002-2021 in patients aged 0-24 due to reflux nephropathy and combined reflux nephropathy with overlapping diagnoses (dysplasia, obstructive uropathies, and other CAKUTs).
Incidence of ESRD from 2002-2021 in patients aged 0-24 due to reflux nephropathy and combined reflux nephropathy with overlapping diagnoses (dysplasia, obstructive uropathies, and other CAKUTs).Incidence of ESRD from 2002-2021 in patients aged 0-24 by all causes.Incidence of ESRD from 2002-2021 in patients aged 0-24 due to reflux nephropathy and combined reflux nephropathy with overlapping diagnoses (dysplasia, obstructive uropathies, and other CAKUTs).