
Nephrology 1
Session: Nephrology 1
 photo")
Eliza Blanchette, MD, MS (she/her/hers)
Assistant Professor
University of Colorado School of Medicine
Denver, Colorado, United States
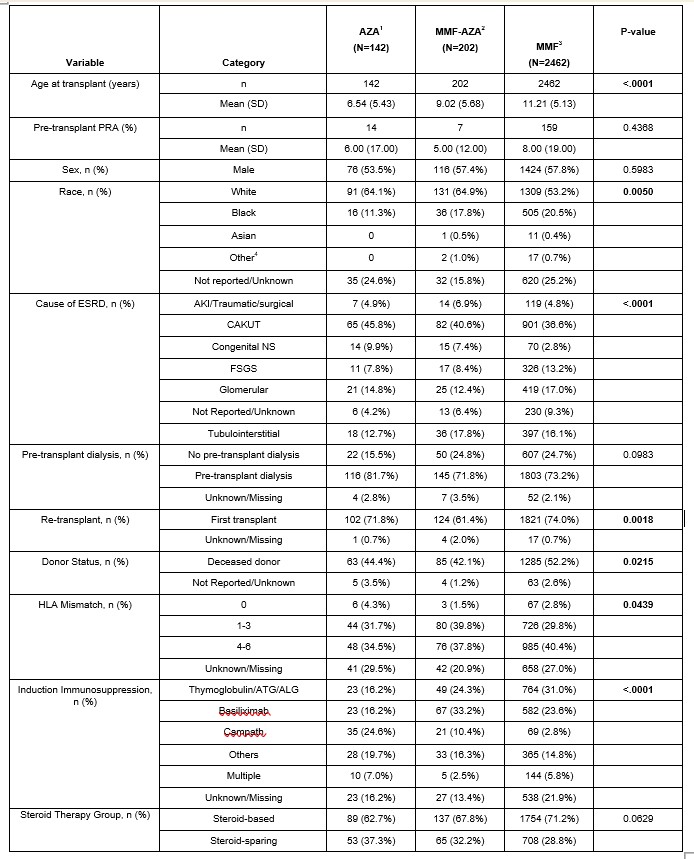 1. AZA group is defined as AZA use at the 30-day post-transplant visit.
1. AZA group is defined as AZA use at the 30-day post-transplant visit. 
 Alemtuzumab induction use is excluded
Alemtuzumab induction use is excluded