
Neonatal Neurology 4
Session: Neonatal Neurology 4
 photo")
Zachary A. Vesoulis, MD MSCI (he/him/his)
Assistant Professor
Washington University School of Medicine
St. Louis, Missouri, United States

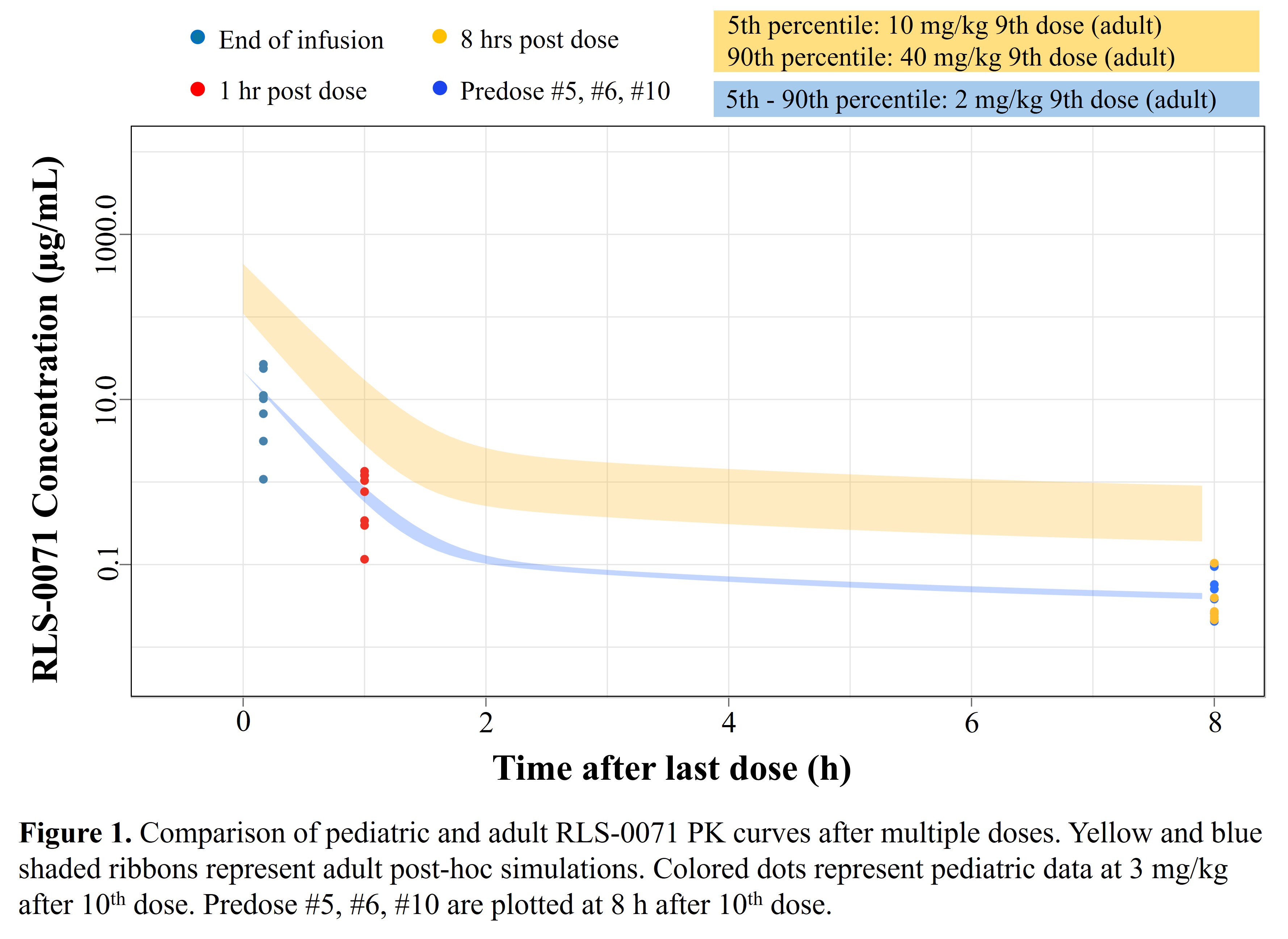 Yellow and blue shaded ribbons represent adult post-hoc simulations. Colored dots represent pediatric data at 3mg/kg after 10th dose. Predose #5, #6, #10 are plotted at 8 hours after 10th dose.Yellow and blue shaded ribbons represent adult post-hoc simulations. Colored dots represent pediatric data at 3mg/kg after 10th dose. Predose #5, #6, #10 are plotted at 8 hours after 10th dose.
Yellow and blue shaded ribbons represent adult post-hoc simulations. Colored dots represent pediatric data at 3mg/kg after 10th dose. Predose #5, #6, #10 are plotted at 8 hours after 10th dose.Yellow and blue shaded ribbons represent adult post-hoc simulations. Colored dots represent pediatric data at 3mg/kg after 10th dose. Predose #5, #6, #10 are plotted at 8 hours after 10th dose.