
Newborn Care 1
Session: Newborn Care 1
 Credit")
 photo")
Tebyan Rabbani, DO (he/him/his)
Fellow
Lucile Packard Children's Hospital Stanford
Palo Alto, California, United States
.jpg) Workflow of biliary atresia screening using direct bilirubin
Workflow of biliary atresia screening using direct bilirubin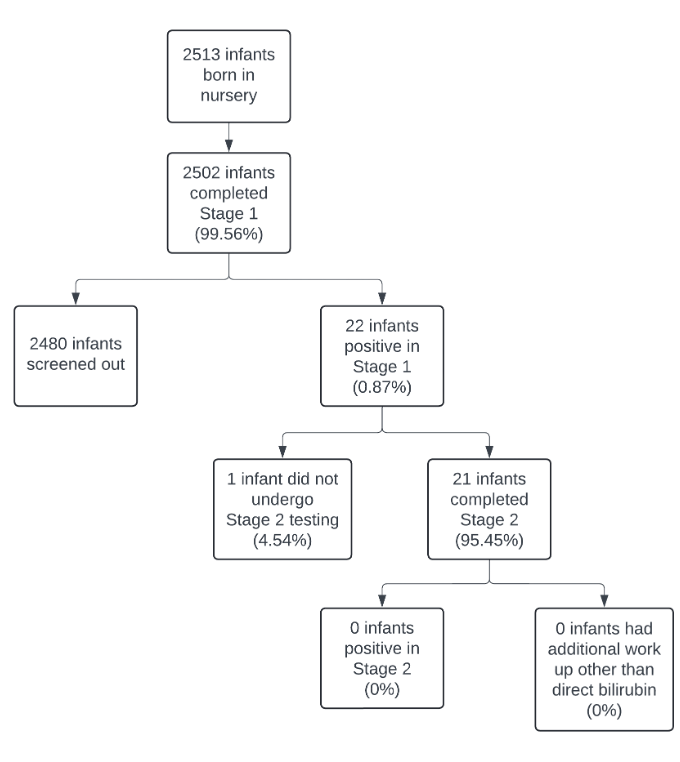 Flow chart depicting outcomes of biliary atresia screening
Flow chart depicting outcomes of biliary atresia screening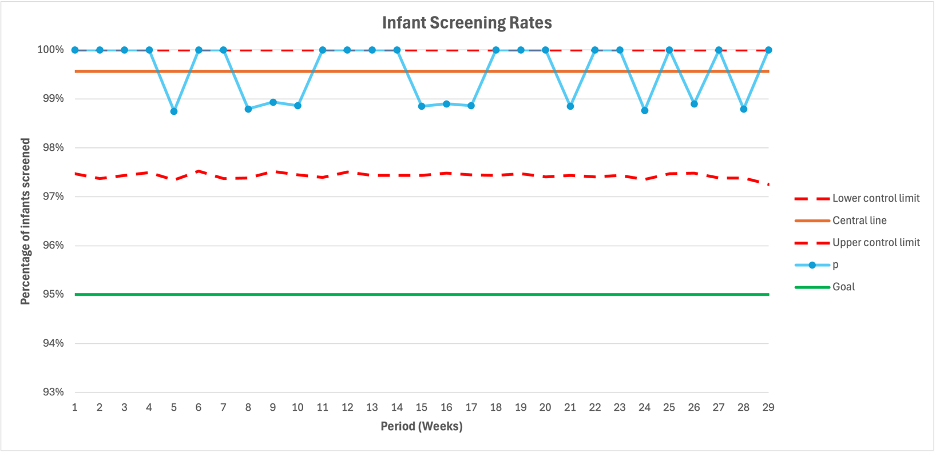 P chart depicting screening rates for biliary atresia
P chart depicting screening rates for biliary atresia