
Palliative Care
Session: Palliative Care
 photo")
Maureen M. Kemna, MD (she/her/hers)
PhD student
University Medical Center Utrecht
Utrecht, Utrecht, Netherlands
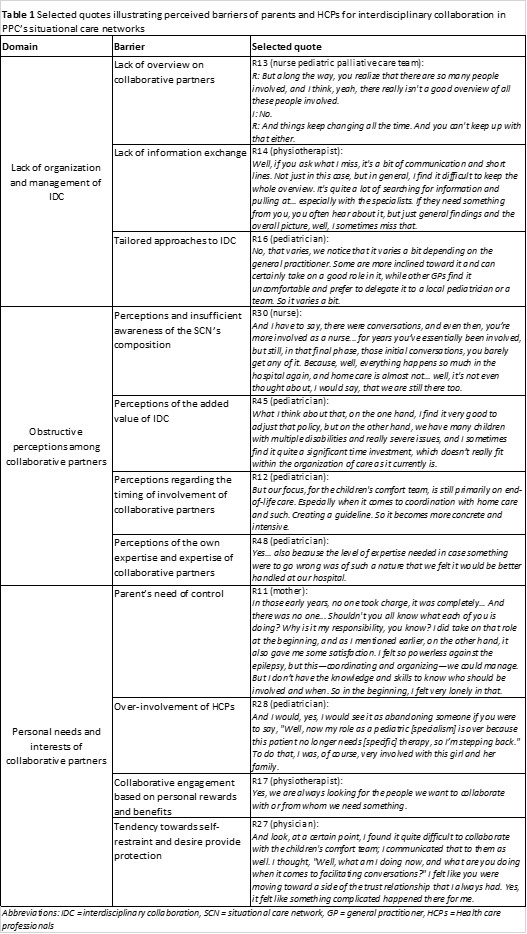 Abbreviations: IDC = interdisciplinary collaboration, SCN = situational care network, GP = general practitioner, HCPs = Health care professionals
Abbreviations: IDC = interdisciplinary collaboration, SCN = situational care network, GP = general practitioner, HCPs = Health care professionals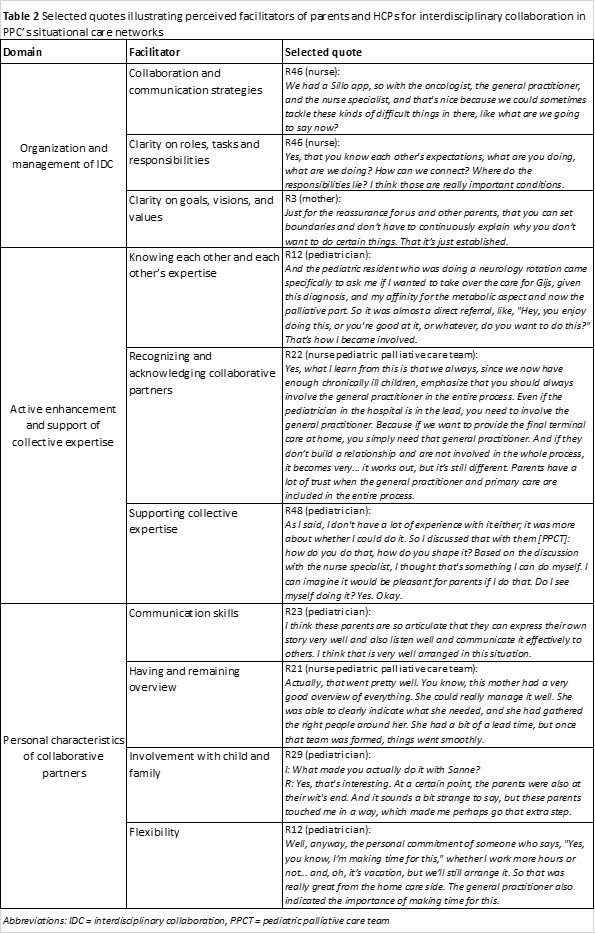 Abbreviations: IDC = interdisciplinary collaboration, PPCT = pediatric palliative care team
Abbreviations: IDC = interdisciplinary collaboration, PPCT = pediatric palliative care team