
Neonatal Neurology 5: Fetal
Session: Neonatal Neurology 5: Fetal
 photo")
Allison J. Chirigos, MD (she/her/hers)
Neonatal and Fetal Neurology Fellow
Cincinnati Children's Hospital Medical Center
Cincinnati, Ohio, United States
.jpg) 5/20 (25%) of survey respondents make the same imaging recommendations regardless of MBM type, with 4 recommending postnatal imaging unconditionally, and 1 recommending imaging conditionally based on the timing of the prenatal magnetic resonance imaging. The other 15/20 (75%) of survey respondents state that their postnatal imaging recommendations differ based on the patient’s MBM type, and this bar graph depicts their recommendations. The green bars represent the number of those 15 providers who recommend cranial ultrasound (CUS), and the blue bars represent the number who recommend magnetic resonance imaging (MRI) for each type of MBM.
5/20 (25%) of survey respondents make the same imaging recommendations regardless of MBM type, with 4 recommending postnatal imaging unconditionally, and 1 recommending imaging conditionally based on the timing of the prenatal magnetic resonance imaging. The other 15/20 (75%) of survey respondents state that their postnatal imaging recommendations differ based on the patient’s MBM type, and this bar graph depicts their recommendations. The green bars represent the number of those 15 providers who recommend cranial ultrasound (CUS), and the blue bars represent the number who recommend magnetic resonance imaging (MRI) for each type of MBM.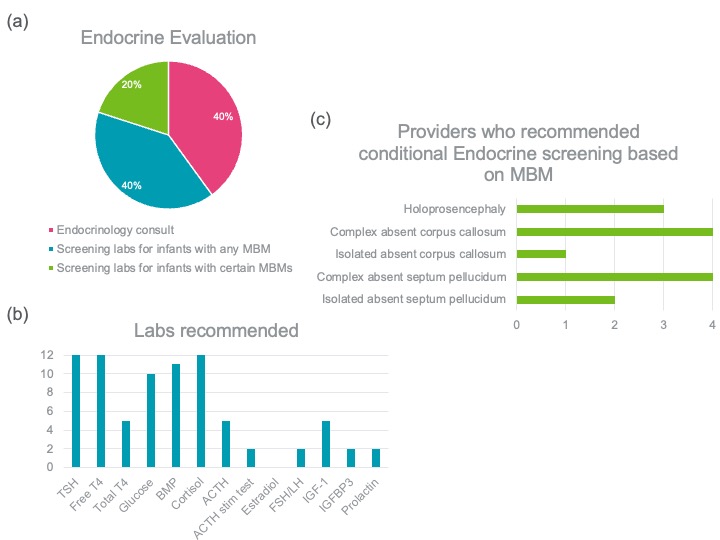 (a) While 20/20 (100%) of providers recommend endocrine screening for patients with MBMs, the pie chart shows the percentage of providers who recommend each screening method. (b) 12/20 (60%) of providers recommend specific screening labs themselves, and the blue bar graph shows the number of providers who recommend each screening lab. (c) 4/20 (20%) of providers recommend endocrine screening conditionally, for patients with certain MBMs. The green bar graph shows the number of providers who recommend endocrine screening by MBM type.
(a) While 20/20 (100%) of providers recommend endocrine screening for patients with MBMs, the pie chart shows the percentage of providers who recommend each screening method. (b) 12/20 (60%) of providers recommend specific screening labs themselves, and the blue bar graph shows the number of providers who recommend each screening lab. (c) 4/20 (20%) of providers recommend endocrine screening conditionally, for patients with certain MBMs. The green bar graph shows the number of providers who recommend endocrine screening by MBM type. 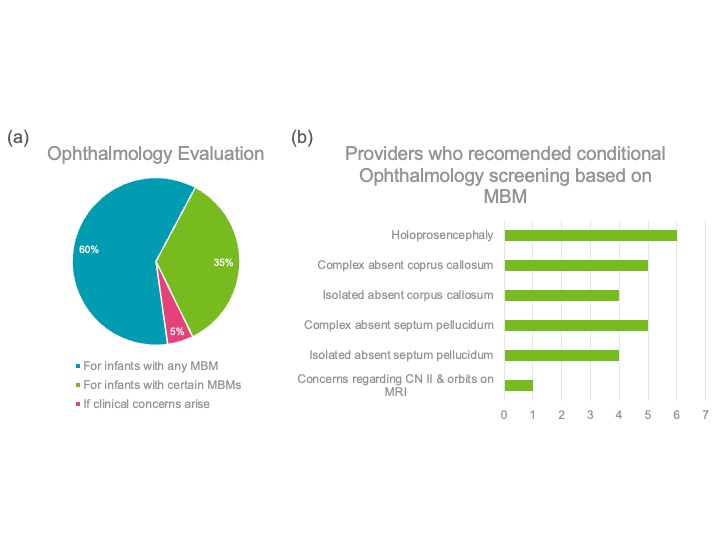 (a) The pie chart shows that while 19/20 (95%) providers recommend ophthalmology evaluation for at least some infants with MBMs, 12/20 (60%) recommend screening for infants with any MBM, and 7/20 (35%) recommend screening for infants with certain MBMs. 1/20 (5%) recommends ophthalmology evaluation only if clinical concerns arise. (b) The bar graph reveals the number of providers who recommend conditional ophthalmology screening based on the MBM.
(a) The pie chart shows that while 19/20 (95%) providers recommend ophthalmology evaluation for at least some infants with MBMs, 12/20 (60%) recommend screening for infants with any MBM, and 7/20 (35%) recommend screening for infants with certain MBMs. 1/20 (5%) recommends ophthalmology evaluation only if clinical concerns arise. (b) The bar graph reveals the number of providers who recommend conditional ophthalmology screening based on the MBM.