
Nephrology 2
Session: Nephrology 2
 photo")
Evan A. Rajadhyaksha, MD (he/him/his)
Fellow
Riley Hospital for Children at Indiana University Health
Indianapolis, Indiana, United States
.jpg) Kruskal-Wallis test revealed a significant difference between groups, comparing ranks (p=0.0005). Means with standard deviation are plotted. Post-hoc Dunn’s multiple comparison p values are denoted between groups.
Kruskal-Wallis test revealed a significant difference between groups, comparing ranks (p=0.0005). Means with standard deviation are plotted. Post-hoc Dunn’s multiple comparison p values are denoted between groups.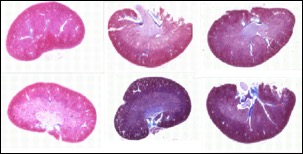 Representative scarring profiles (Masson’s trichrome), displaying 25th and 75th percentile scars for each group.
Representative scarring profiles (Masson’s trichrome), displaying 25th and 75th percentile scars for each group.