
Neonatal Neurology 4
Session: Neonatal Neurology 4
 photo")
Srinivas Kota, PhD (he/him/his)
Assistant Professor
University of Texas Southwestern Medical School
Dallas, Texas, United States
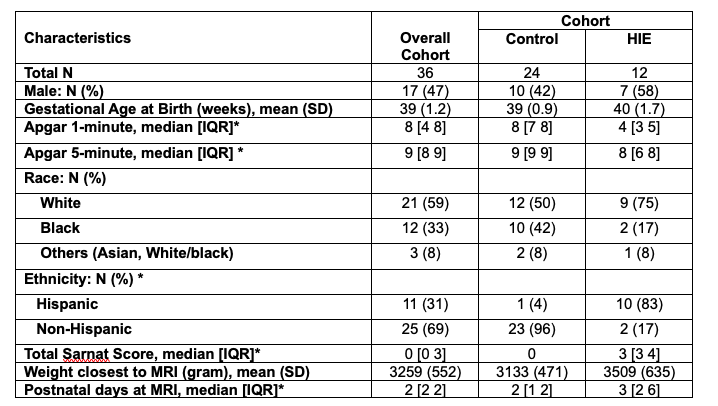 Neonatal characteristics of the healthy control and HIE cohorts
Neonatal characteristics of the healthy control and HIE cohorts 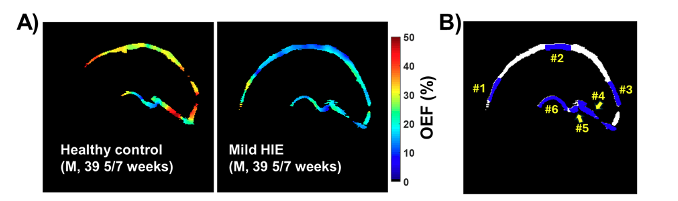 A) Representative oxygen extraction fraction (OEF) maps from a healthy control and the age and gender-matched neonate with mild HIE. B) Example of the regions-of-interest (ROIs) used in OEF quantification include 1) frontal superior sagittal sinus, 2) middle sagittal sinus, 3) posterior sagittal sinus, 4) straight sinus, 5) vein of Galen, and 6) internal cerebral vein.
A) Representative oxygen extraction fraction (OEF) maps from a healthy control and the age and gender-matched neonate with mild HIE. B) Example of the regions-of-interest (ROIs) used in OEF quantification include 1) frontal superior sagittal sinus, 2) middle sagittal sinus, 3) posterior sagittal sinus, 4) straight sinus, 5) vein of Galen, and 6) internal cerebral vein.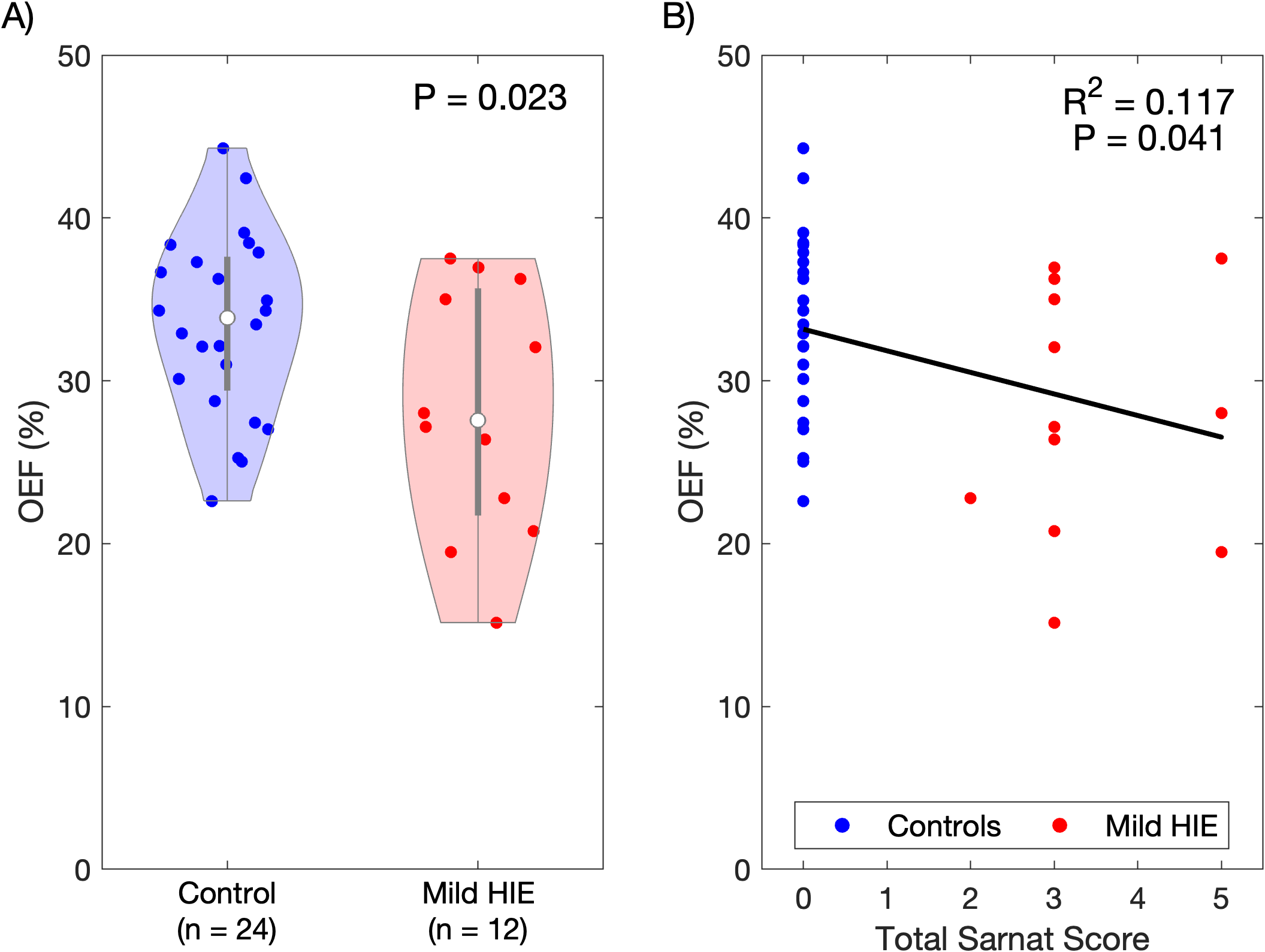 Figure 2 A) Distribution of global cortical oxygen extraction fraction (OEF) for newborns with mild HIE and healthy controls, with significant differences observed (P = 0.023) using the Student t-test. B) OEF is significantly negatively correlated with Total Sarnat Score (regression coefficient = -1.325, R² = 0.117, P = 0.041). Black line indicates the linear regression fit. Neonatal characteristics of the healthy control and HIE cohorts A) Representative oxygen extraction fraction (OEF) maps from a healthy control and the age and gender-matched neonate with mild HIE. B) Example of the regions-of-interest (ROIs) used in OEF quantification include 1) frontal superior sagittal sinus, 2) middle sagittal sinus, 3) posterior sagittal sinus, 4) straight sinus, 5) vein of Galen, and 6) internal cerebral vein.Figure 2 A) Distribution of global cortical oxygen extraction fraction (OEF) for newborns with mild HIE and healthy controls, with significant differences observed (P = 0.023) using the Student t-test. B) OEF is significantly negatively correlated with Total Sarnat Score (regression coefficient = -1.325, R² = 0.117, P = 0.041). Black line indicates the linear regression fit.
Figure 2 A) Distribution of global cortical oxygen extraction fraction (OEF) for newborns with mild HIE and healthy controls, with significant differences observed (P = 0.023) using the Student t-test. B) OEF is significantly negatively correlated with Total Sarnat Score (regression coefficient = -1.325, R² = 0.117, P = 0.041). Black line indicates the linear regression fit. Neonatal characteristics of the healthy control and HIE cohorts A) Representative oxygen extraction fraction (OEF) maps from a healthy control and the age and gender-matched neonate with mild HIE. B) Example of the regions-of-interest (ROIs) used in OEF quantification include 1) frontal superior sagittal sinus, 2) middle sagittal sinus, 3) posterior sagittal sinus, 4) straight sinus, 5) vein of Galen, and 6) internal cerebral vein.Figure 2 A) Distribution of global cortical oxygen extraction fraction (OEF) for newborns with mild HIE and healthy controls, with significant differences observed (P = 0.023) using the Student t-test. B) OEF is significantly negatively correlated with Total Sarnat Score (regression coefficient = -1.325, R² = 0.117, P = 0.041). Black line indicates the linear regression fit. 