
Asthma 2
Session: Asthma 2
 photo")
Tamara Perry, MD (she/her/hers)
Professor of Pediatrics and Chief of Allergy/Immunology
University of Arkansas for Medical Sciences College of Medicine
Little Rock, Arkansas, United States
.png) Figure 1. Proportion of participants in the PEAKmAAP (with or without DS) and UC groups with ACT >19. The PEAKmAAP group had a higher proportion of participants with ACT >19 over the 12-month intervention period with a statistically significant difference by 12 months.
Figure 1. Proportion of participants in the PEAKmAAP (with or without DS) and UC groups with ACT >19. The PEAKmAAP group had a higher proportion of participants with ACT >19 over the 12-month intervention period with a statistically significant difference by 12 months.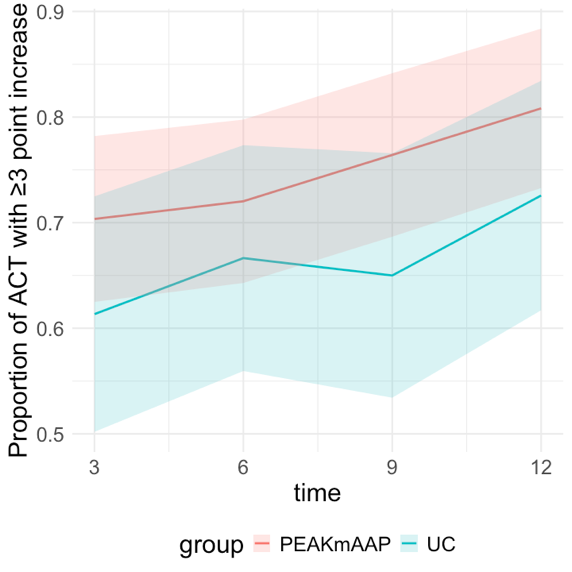 Figure 2. Proportion of participants with a clinically significant increase in ACT score (≥3-point increase compared to baseline) in the PEAKmAAP and UC groups. No statistically significant differences were seen between PEAKmAAP groups and UC.
Figure 2. Proportion of participants with a clinically significant increase in ACT score (≥3-point increase compared to baseline) in the PEAKmAAP and UC groups. No statistically significant differences were seen between PEAKmAAP groups and UC.