
Neonatal Clinical Trials 1
Session: Neonatal Clinical Trials 1
 photo")
Courtney Hallock (she/her/hers)
Student
University of Washington School of Medicine
Bozeman, Montana, United States
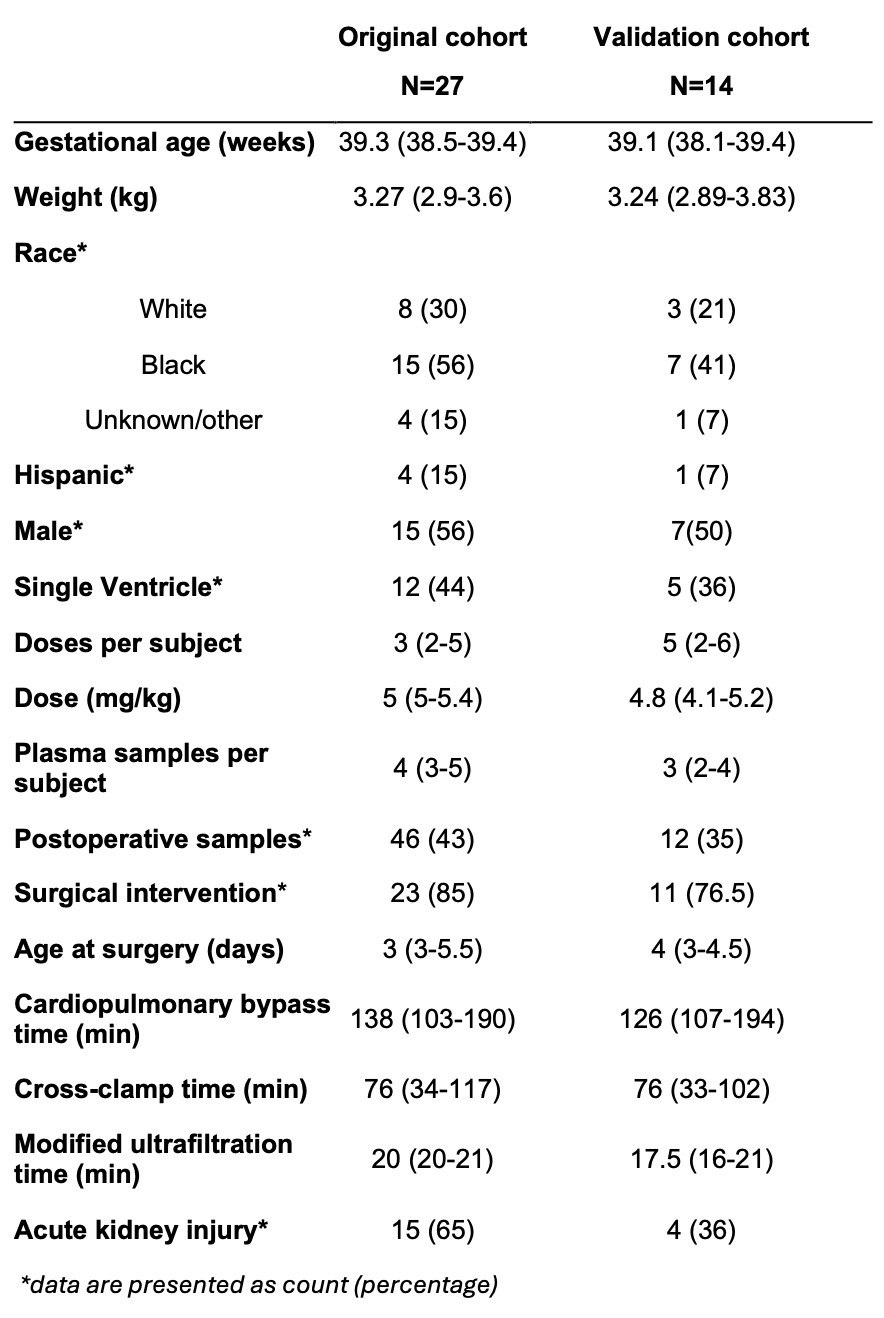 Demographic and clinical characteristics of the original and validation cohorts, presented as median (25th-75th percentile).
Demographic and clinical characteristics of the original and validation cohorts, presented as median (25th-75th percentile).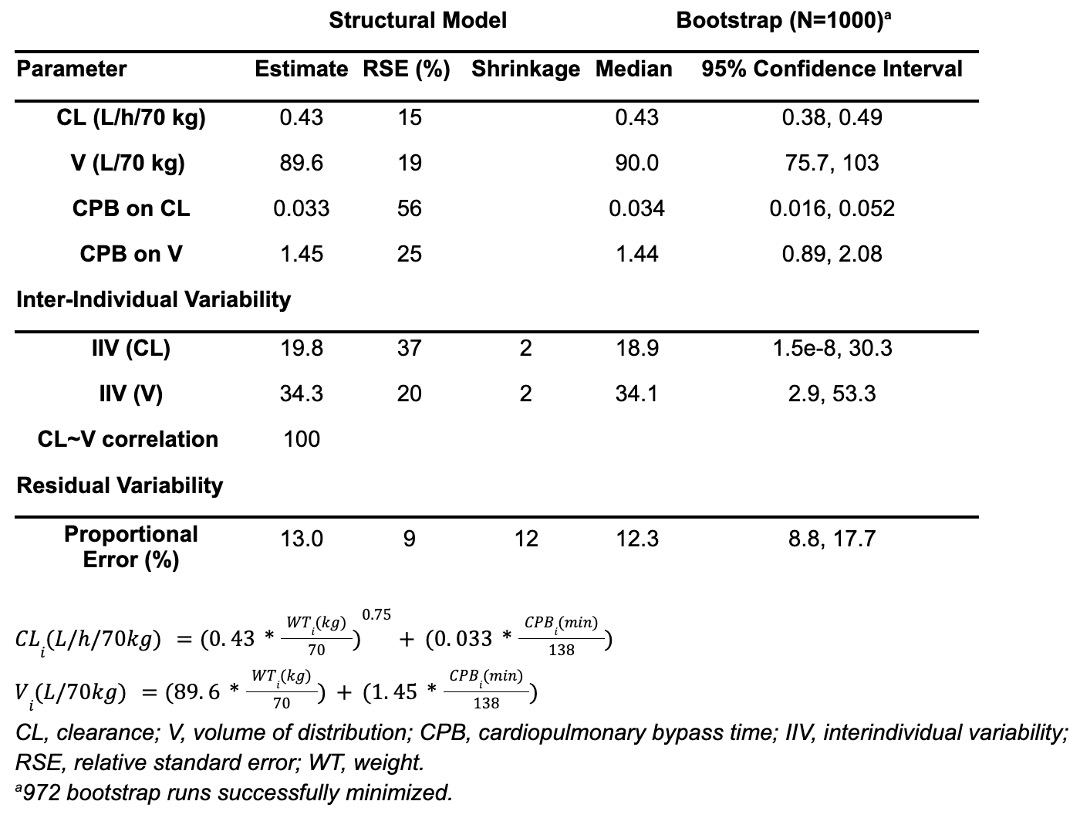 Original population pharmacokinetic model parameter estimates and bootstrap results.
Original population pharmacokinetic model parameter estimates and bootstrap results.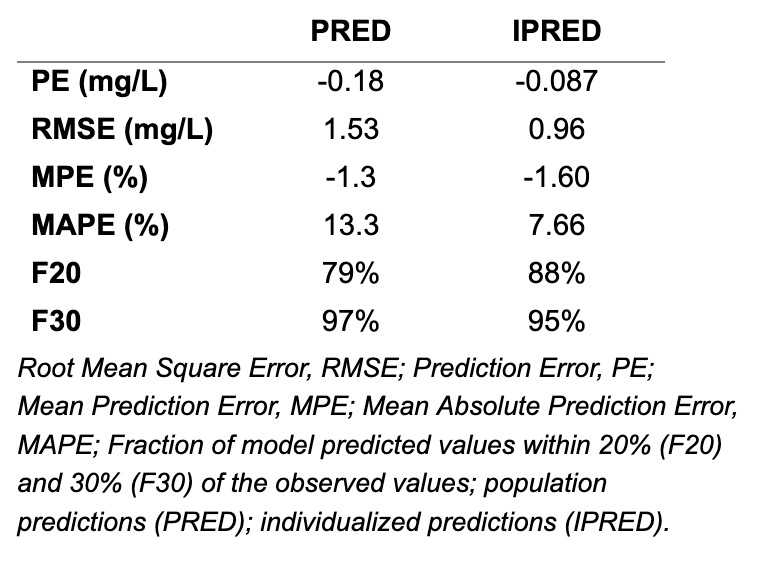 Assessment of model precision and accuracy.
Assessment of model precision and accuracy.