
Neonatal Neurology 4
Session: Neonatal Neurology 4

Daniel Diatlov, MSc
Medical Student
Stanford University School of Medicine
Stanford, California, United States
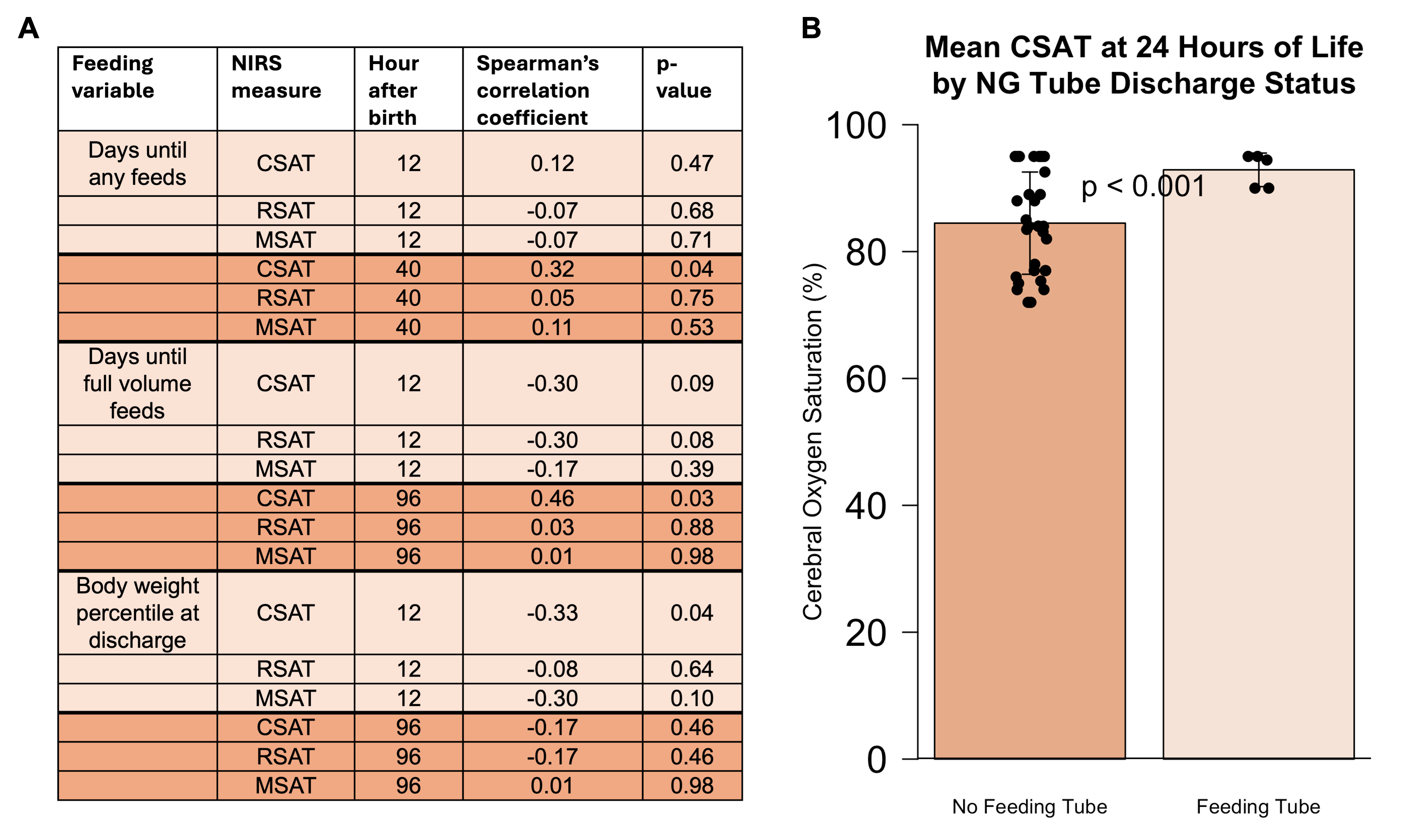 (A) Summary of correlations between feeding outcomes and NIRS measures at early and late time points. (B) Association between CSAT value and feeding tube discharge status at 24 hours of life (p=0.0002).
(A) Summary of correlations between feeding outcomes and NIRS measures at early and late time points. (B) Association between CSAT value and feeding tube discharge status at 24 hours of life (p=0.0002). 