
Nephrology 1
Session: Nephrology 1
 photo")
Elizabeth A. Onugha, MD MSCI (she/her/hers)
Assistant Professor
Baylor College of Medicine
The Woodlands, Texas, United States
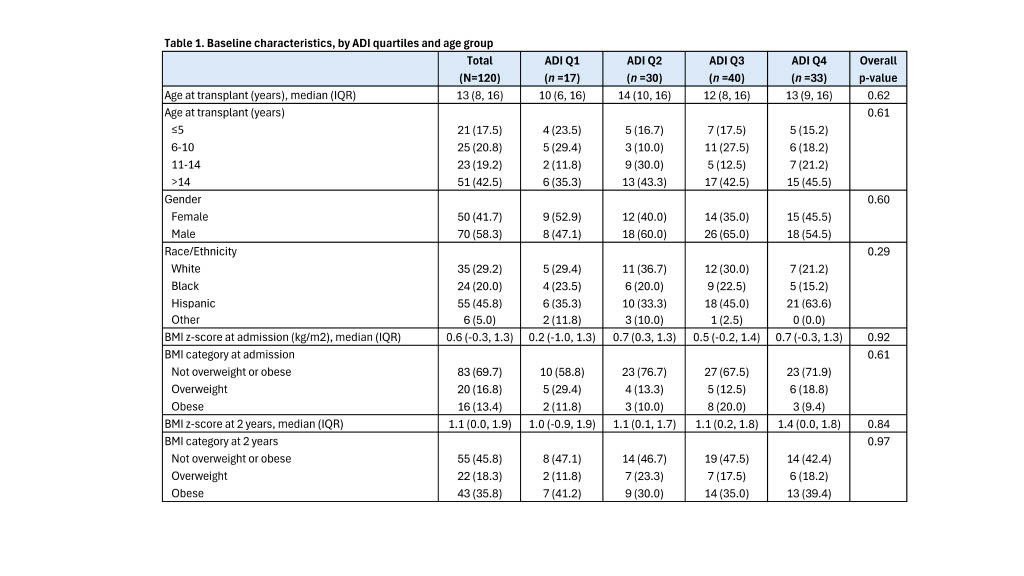 Baseline characteristics, by ADI quartiles and age group
Baseline characteristics, by ADI quartiles and age group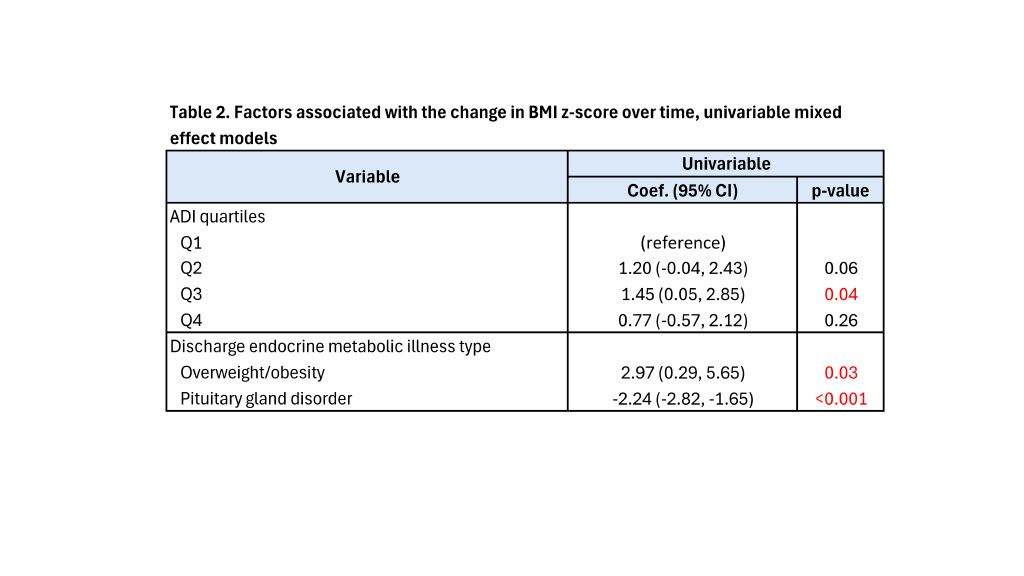 Factors associated with the change in BMI z-score over time, univariable mixed effect models
Factors associated with the change in BMI z-score over time, univariable mixed effect models