
Neonatal Clinical Trials 1
Session: Neonatal Clinical Trials 1
 photo")
Souvik Mitra, MD, PhD, FRCPC, DRCPSC (he/him/his)
Associate Professor
University of British Columbia Faculty of Medicine
Vancouver, British Columbia, Canada
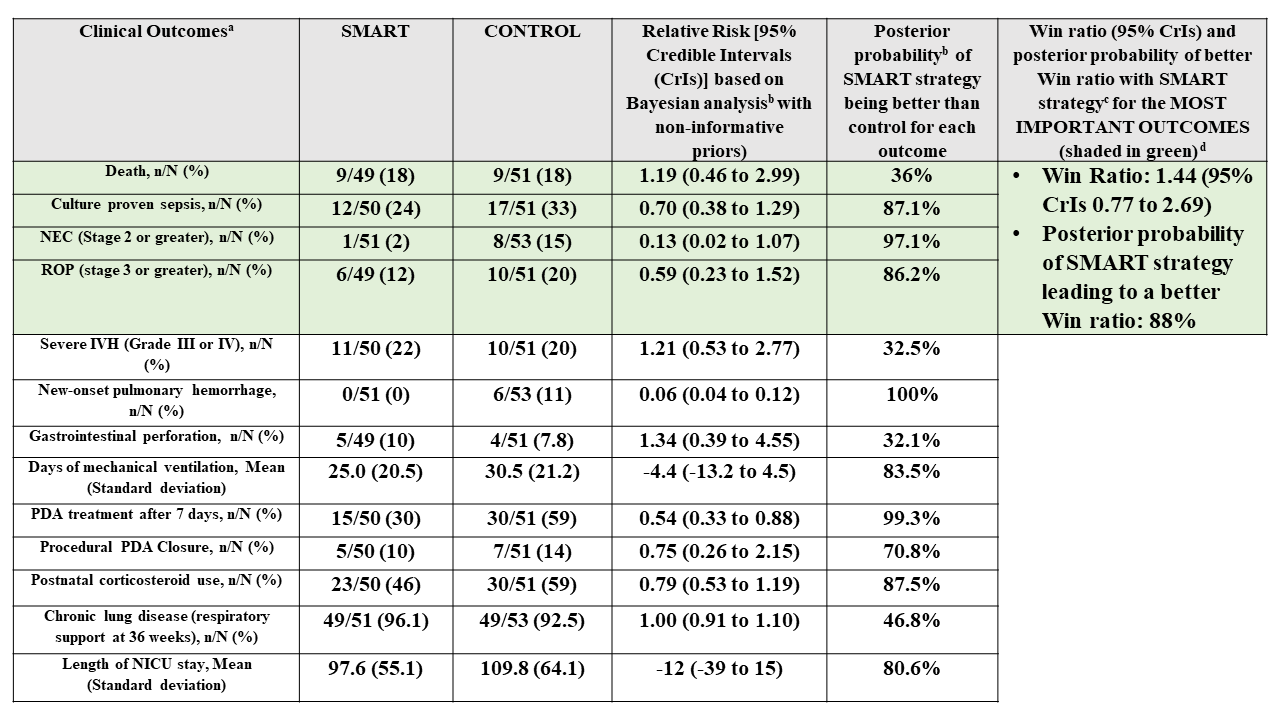 (a) Outcome data based on preliminary analysis of available completed data at time of abstract submission. Final numbers may change prior to presentation/publication;
(a) Outcome data based on preliminary analysis of available completed data at time of abstract submission. Final numbers may change prior to presentation/publication;